The societal burden of the opioid crisis estimated at $1 trillion in 2017
Understanding the magnitude of the opioid crisis in terms of both the overall economic impact and the distribution of this impact across different sectors is important for decision-makers in implementing interventions and policies. Studies measuring the societal economic burden of substance use disorder as well as harmful and hazardous substance use typically use three components: increased healthcare costs, increased criminal justice costs, and lost productivity costs (e.g., sick time; disability; unemployment). In this study, researchers examined the economic burden of the opioid crisis in 2017 using a novel method that accounts for the economic burden of both reduced quality of life from opioid use disorder and premature deaths from fatal opioid overdoses.
The opioid crisis has claimed nearly 450,000 lives in the last 20 years, with recent evidence showing that overdose deaths reached an all-time highin 2019 and preliminary evidence suggesting that the coronavirus pandemic has further exacerbated these deaths. Understanding the overall economic impact of the opioid crisis is crucial in drawing public attention to it, increasing political will, and in mobilizing and investing in necessary resources to address it and curb costs. In addition, decision-makers need to know how specific parts of the economy are affected by opioid-related harms. For example, employers will be interested in how the productivity of their workers is affected whereas criminal justice stakeholders might be interested in the cost to correctional facilities.
Economic cost analyses assume different stakeholder perspectives (e.g., taxpayer, government, health insurer) when estimating overall costs. In a cost-of-illness study, such as one that comprehensively measures the economic impact of opioid use disorders and their consequences, a societal perspective is usually employed.
This perspective includes the overall costs to society, incorporating multiple perspectives such as those of an individual, the government, and the healthcare system. Previous studies that have measured the economic burden of the opioid crisis using a societal perspective typically use a “human capital” approach. This approach typically accounts for healthcare costs, criminal justice costs, and lost productivity, including the loss of wages from premature fatalities. In this study, researchers use the ‘value of a statistical life’ instead of the ‘human capital’ approach to measure morbidity and mortality, substantially increasing the economic burden estimates of opioid use disorder and fatal opioid overdoses compared with previous studies. This method was first used by the Council of Economic Advisors and recognizes that premature fatalities have value beyond their more direct economic impact. Accounting for premature fatalities, using the value of a statistical life, and reduced quality of life from opioid use disorder using the value of a statistical life year, may give a more accurate representation of the total societal welfare loss due to the opioid crisis and better-inform efforts to prevent opioid use disorder and reduce the rate of fatal opioid overdoses.
HOW WAS THIS STUDY CONDUCTED?
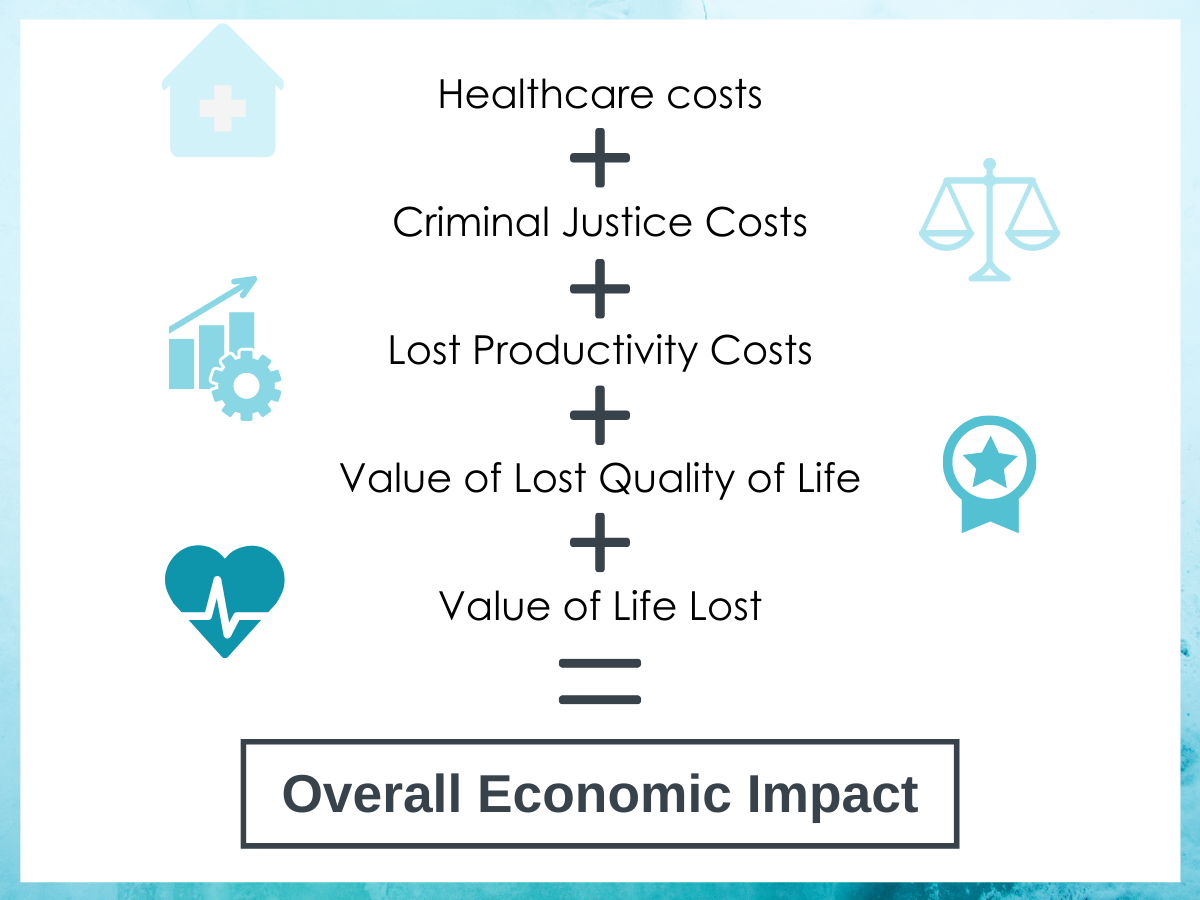
This economic analysis used a societal perspective to estimate the nonfatal and fatal costs of the opioid crisis in 2017, with specific measurements for healthcare, criminal justice, and lost productivity. The cost of morbidity resulting from reduced quality of life was measured by the value of a statistical life year ($517,324), and the cost of premature mortality resulting from fatal overdose death was measured by the value of a statistical life ($10.1 million). See below for more detail on how each of these economic impacts were calculated.
Researchers obtained the incidence of fatal opioid overdoses through the National Vital Statistics System and the prevalence of opioid use disorder from the National Survey on Drug Use and Health. According to these data sources, there were 47,600 opioid overdose deaths and 2.13 million people with opioid use disorder in the United States in 2017. Guidelines from the United States Department of Health and Human Services were used to measure morbidity and mortality using the ‘value of a statistical life’ approach. Economic costs were measured in the following categories:
Healthcare: Researchers used a methodology from a previous study to measure the impact of opioid use disorder diagnoses on healthcare spending. This previous study used a claims database to estimate the increased annual healthcare costs associated with opioid use disorder for commercial, Medicaid, and Medicare beneficiaries. The increased costs for each type of insurance beneficiary was then multiplied by the number of people with opioid use disorder derived from the National Survey on Drug Use and Health for each insurance coverage category. To account for opioid use disorder treatment that is not funded by health insurance, federal, state, local, and private expenditures on substance use disorder treatment were identified through SAMHSA. This total was multiplied by the ratio of cases of opioid use disorder among all those with substance use disorder derived from the 2017 National Survey on Drug Use and Health.
Criminal Justice: Researchers divided these costs up by police protection, legal and adjudication, correctional facilities, and property lost due to crimes. The total costs for police protection and legal and adjudication was multiplied by the percentage that was drug related. Then, this figure was multiplied by the ratio of cases of opioid use disorder among all those with a drug use disorder (which included all types of substance use disorders other than alcohol) derived from the 2017 National Survey on Drug Use and Health. The total cost for correctional facilities was calculated by multiplying the cost for those incarcerated with drug-related crimes by the ratio of cases of opioid use disorder among all those with a drug use disorder. Property lost due to crimes was derived from total drug-related property loss multiplied by the ratio of cases of opioid use disorder among all those with a drug use disorder.
Lost Productivity: Researchers used a methodology from a previous study extending to both illicit and prescription opioids. Lost productivity comes from three sources: reduced productive hours from opioid use disorder, incarceration related to opioids, and premature death from opioid overdose. For lost productivity from opioid use disorder, the percentage reduction in productivity attributable to this disorder (17% for males and 18% for females) was multiplied by the average annual production value of the U.S. population and the national prevalence of opioid use disorder from National Survey on Drug Use and Health, taking into account age and gender. For lost productivity from incarceration, the number of those incarcerated for crimes attributable to opioid use disorder were multiplied by the average annual production value of the U.S. population. For premature death from opioid overdose, the value of lost salary and fringe benefits as well as the loss of household production were estimated in a cost module from the CDC.
Valuation of Lost Quality of Life: First, the difference between the health-related quality of life for a person with and without opioid use disorder was calculated using the findings of a previous study. This difference varied based on if a person was an injection drug user, had a prescription opioid use disorder, or had recently initiated treatment. To measure the total valuation due to reduced quality of life, the prevalence of those with opioid use disorder from the National Survey on Drug Use and Health that met each of these categories was multiplied by the reduction in health-related quality of life and then by the value of a statistical life year ($517,324). Valuation of lost quality of life represents a measure of the morbidity of opioid use disorder.
Values of Life Lost: The value of a statistical life ($10.1 million) was multiplied by the number of opioid overdose deaths in 2017 to calculate the value of life lost. Value of life lost represents a measure of the mortality from opioid use disorder, opioid misuse, and opioid use.
The cost in each of these five categories was added together for the total valuation of economic burden of opioid use disorder and fatal overdose. This total valuation was also broken down into nonfatal and fatal costs.
Figure 1.
Previous literature has suggested that opioid use disorder prevalence is underestimated and opioid overdoses as a share of all drug overdose deaths is undercounted. In addition, it is recommended that the value of a statistical life method should provide a low-end and high-end cost. This study also uses data from a variety of sources. Given these variations, the researchers conducted sensitivity analyses using alternative assumptions to test the robustness of their results.
WHAT DID THIS STUDY FIND?
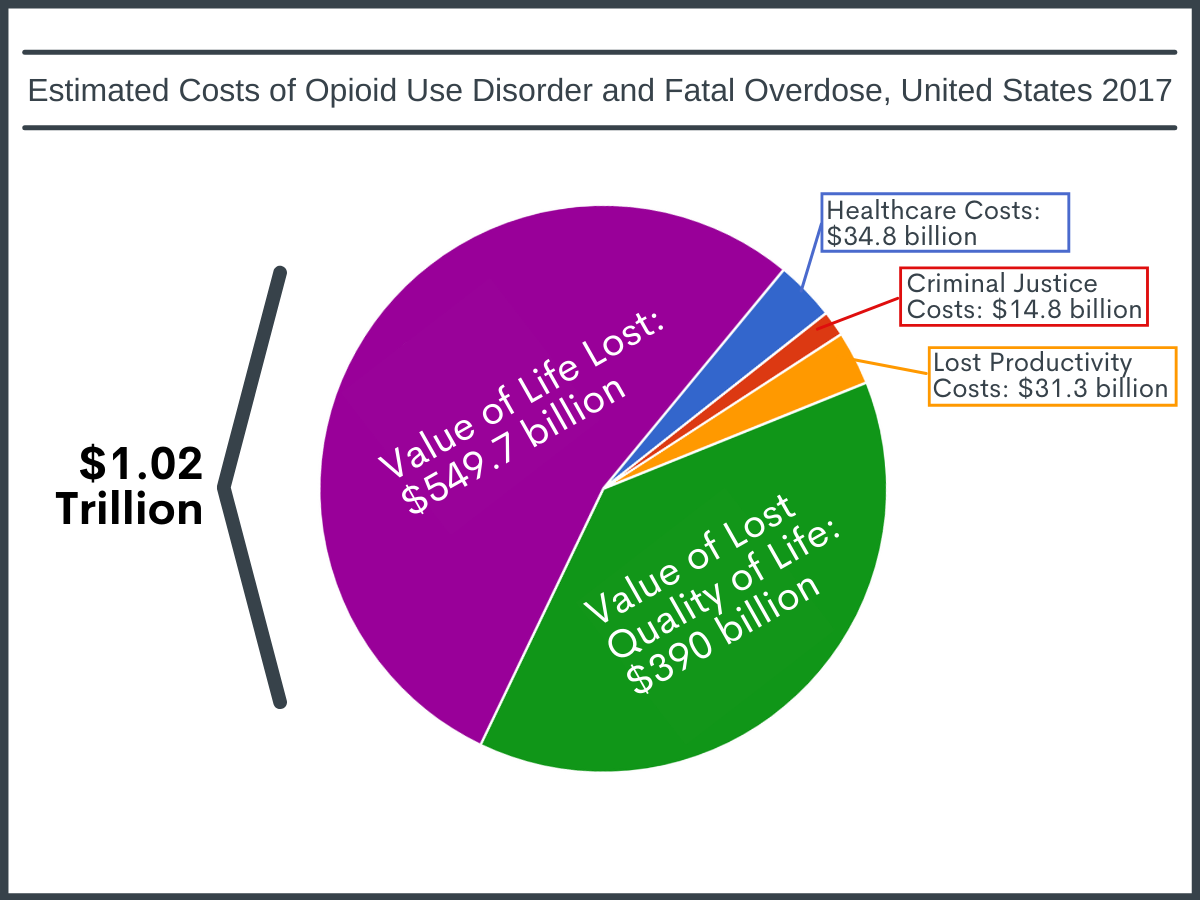
The overall estimated cost of the opioid crisis in 2017 was $1.02 trillion.
A slightly lower amount of this economic burden was attributable to costs related to opioid-related harms ($471 billion) when compared to costs related to opioid-involved deaths ($550 billion).
Most of the costs are from morbidity and mortality.
Over 85% of the total economic burden was from the value of the reduced quality of life from opioid use disorder ($391 billion) and the value of life lost to opioid overdose ($481 billion).
Lost productivity costs were higher than healthcare and criminal justice costs.
Total lost productivity costs amounted to $100 billion and included the nonfatal costs of $23.5 billion due to reduced productivity from opioid use disorder and $7.8 billion due to lost productivity from incarceration, as well as the fatal costs of $68.7 billion due to forgone wages from premature fatality. The cost to healthcare was $34.8 billion, which included $12.9 to private insurance, $11.1 to Medicaid, $3.2 billion to Medicare, and $3.5 billion from funding outside of health insurance. Criminal justice costs amounted to $14.8 billion, with police protection ($6.2 billion) and correctional facilities ($5.4 billion) bearing the largest burden.
Figure 2. Full breakdown of total economic burden in this analysis.
Sensitivity analyses place the economic burden as low as $500 billion and as high as $1.5 trillion.
When different valuations or weights were considered and different assumptions were made about opioid use disorder prevalence and the number of opioid overdose deaths, estimates ranged between $500 billion and $1.5 trillion. The largest fluctuations were seen when using alternative values (low-end and high-end estimates) for a statistical life and alternative weights for health-related quality of life.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that the overall estimated cost of opioid use disorder and fatal opioid overdoses was $1.02 trillion in 2017, with 85% of this burden from the value of the reduced quality of life from opioid use disorder and life lost to opioid overdose, while lost productivity was estimated at $100 billion, healthcare costs were estimated at $34.8 billion, and criminal justice costs estimated at $14.8 billion.
These findings suggest that a substantial amount of value in the U.S. economy is lost due to the opioid crisis, highlighting that considerable economic benefits can be reaped from a two-pronged approach of preventing opioid use disorder and reducing the rate of fatal opioid overdoses. In fact, a recent study using a similar methodology estimates that preventing one case of opioid use disorder would save society $2.2 million. Strategies to prevent opioid use disorder include interventions and policies to promote cautious prescribing of opioids such as prescription drug monitoring programs and state prescription drug laws, safe storage and disposal of prescription opioids, and early interventionof prescription opioid misuse. Also, primary prevention of opioid misuse may be part of evidence-based prevention in children and teens that targets enhanced social and developmental skills.
In addition to preventing opioid use disorder, there are several treatment and harm reduction strategies that have been shown to reduce opioid overdose deaths, lessening the economic burden of the opioid crisis. Medications for opioid use disorder, especially opioid agonists such as methadone and buprenorphine, have been shown to reduce overdose mortality for those with an opioid use disorder. Emerging evidence suggests that initiation of these medications in certain settings, such as emergency departmentsand the criminal justice system, have the potential to reduce mortality substantially. Other promising models for initiation include post-overdose response teams and peer outreach. In addition to initiation, strategies for retaining individuals on medications for opioid use disorder are crucial to improve long-term outcomes. High-risk individuals and their family members should have access to naloxone, an opioid overdose antidote, which has been shown to be one of the most effective strategies in reducing opioid overdose mortality. Given the human and economic toll of the opioid crisis, more innovative yet controversial approaches might be considered, including drug checking services, safe consumption sites, and safe drug supply.
Although the reduction in quality of life from opioid use disorder and life lost to opioid overdose, as measured by the value of a statistical life, made up the large majority of the economic costs attributable to the opioid crisis, lost productivity ($100 billion), increased healthcare costs ($34.8 billion), and increased criminal justice costs ($14.8 billion) were sizeable. Lost productivity may directly affect employers and indirectly affect the government, through lost tax revenues. Employer-led initiatives, such as recovery friendly workplaces, hold promise. Stakeholders in the healthcare system and the criminal justice system may benefit from implementing many of the strategies already discussed to prevent opioid use disorder and reduce overdose mortality.
Some of the creative efforts to capture all costs associated with an illness can become more of an art than a science. This is especially true regarding the new methodology employed by this study to measure premature fatalities and reduced quality of life using the value of a statistical life.
Previous studies have primarily used a ‘human capital’ approach, which totals the economic loss of a premature fatality by measuring lost economic output. The ‘value of a statistical life’ approach is typically used in policy analyses as a willingness-to-pay for risk reduction by individuals or society.
Used in a cost-of-illness analysis, the ‘value of a statistical life’ approach will result in a much higher total economic cost than the ‘human capital’ approach. However, the true economic toll of reduced quality of life and premature fatality from the opioid crisis is likely to fall somewhere between these two approaches.
Given that measuring the societal economic burden of substance-related harms has historically used a ‘human capital’ approach, the ‘value of a statistical life’ approach could serve as a model for understanding the ‘true’ costs of other substances, especially alcohol, which carries the largest public health burden because of its wide availability, normalized use, toxicity, and the presence of a profit-maximizing industry that markets its use. More research is needed to determine which methodology more accurately captures the overall economic burden of the opioid crisis and how this methodology might translate to other substances.
Typically, cost-of-illness studies use a ‘human capital’ approach in measuring the economic valuation of morbidity and mortality. Adding the value of a statistical life to measure valuation beyond economic output, which accounts for 85% of the total burden in this study, may overestimate the actual economic impact of the opioid crisis possibly leading to some stakeholders discrediting economic cost burden analyses.
The ratio of opioid use disorder cases among those with a substance use disorder or drug use disorder (all substance use disorders except alcohol) was used for many of the calculations. However, certain types of substances may disproportionately affect costs. For instance, criminal justice costs may be higher on average for people with opioid use disorder compared to people with a cannabis use disorder, both considered types of drug use disorders.
This study uses averages across the entire United States population which may not be representative of the population with opioid use disorder. For example, the societal willingness to pay, or the value of a statistical life, may be different for preventing a fatal opioid overdose than the general value used in this study. Also, the average earnings of the U.S. population may not be representative of the earnings for those with opioid use disorder.
There is uncertainty in the national prevalence of opioid use disorder and the share of opioid overdose deaths among all drug overdose deaths. Though a higher share of opioid overdose deaths is accounted for in sensitivity analyses, the study does not examine the likely scenario that national opioid use disorder prevalence is twofold or more higher than that reported by the National Survey on Drug Use and Health.
Some ripple effects of the opioid crisis are not captured in this economic analysis, such as the healthcare costs of neonatal abstinence syndrome and the reduced quality of life experienced by family members of those with opioid use disorder.
Most opioid overdose deaths have an additional non-opioid substance present on the toxicology report and most people with opioid use disorder use multiple substances. Therefore, it is difficult to attribute the economic costs in this study entirely to opioids.
This study appears to take a ‘value of a statistical life’ approach to measuring the economic loss of premature fatality rather than a ‘human capital’ approach. However, lost productivity is included as a fatal cost in the economic analysis, likely double counting the economic loss due to premature fatality.
BOTTOM LINE
This study found that the overall estimated cost of opioid use disorder and fatal opioid overdoses was $1.02 trillion in 2017, with 85% of this burden from the value of the reduced quality of life from opioid use disorder and life lost to opioid overdose, while lost productivity was estimated at $100 billion, healthcare costs were estimated at $34.8 billion, and criminal justice costs estimated at $14.8 billion.
For individuals and families seeking recovery: In addition to the human toll, the opioid crisis has a substantial economic impact. Safe storage and disposal of prescription opioids is one way to prevent prescription opioid misuse and opioid use disorder. Medications for opioid use disorder, such as buprenorphine, methadone, and extended-release naltrexone, have been shown to be effective treatment options. Individuals at high-risk for opioid overdose and their families also should have access to naloxone in case of emergency.
For treatment professionals and treatment systems: There are substantial economic benefits from implementing evidence-based interventions that prevent opioid use disorder and reduce opioid overdose deaths, in addition to improving clinical outcomes. Some of these interventions may include early intervention for prescription opioid misuse, having the capacity to provide medications for opioid use disorder when indicated, distributing naloxone to high-risk individuals, and linkage to local harm reduction services such as syringe service programs.
For scientists:This cost-of-illness study uses a new methodology to assess reduced quality of life and premature fatality, the value of a statistical life, which goes beyond measuring an individual’s economic output. This methodology would benefit from future research to examine if a measure typically used in policy analyses as a willingness-to-pay for risk reduction is more accurate in capturing overall economic costs in a cost-of-illness study compared with the human capital approach. The findings of this study show that there are substantial economic benefits of preventing opioid use disorder and reducing opioid overdose deaths, highlighting the need for evaluating policies and interventions based on these outcomes.
For policy makers: There are substantial economic benefits to be reaped from implementing evidence-based interventions and policies that prevent opioid use disorder and reduce opioid overdose deaths. Interventions to ensure cautious opioid prescribing, such as prescription drug monitoring programs, academic detailing, and state prescription drug laws, can prevent the onset of new cases of opioid use disorder. Emerging evidence suggests that policies to expand the availability of medications for opioid use disorder and naloxone in high-risk settings, such as emergency departments and the criminal justice system, can reduce opioid overdose deaths. Given the human and economic toll of the opioid crisis, more innovative approaches that are utilized in other industrialized nations but have proved more controversial in the United States might be considered, including drug checking services, safe consumption sites, and safe drug supply.
The opioid crisis has claimed nearly 450,000 lives in the last 20 years, with recent evidence showing that overdose deaths reached an all-time highin 2019 and preliminary evidence suggesting that the coronavirus pandemic has further exacerbated these deaths. Understanding the overall economic impact of the opioid crisis is crucial in drawing public attention to it, increasing political will, and in mobilizing and investing in necessary resources to address it and curb costs. In addition, decision-makers need to know how specific parts of the economy are affected by opioid-related harms. For example, employers will be interested in how the productivity of their workers is affected whereas criminal justice stakeholders might be interested in the cost to correctional facilities.
Economic cost analyses assume different stakeholder perspectives (e.g., taxpayer, government, health insurer) when estimating overall costs. In a cost-of-illness study, such as one that comprehensively measures the economic impact of opioid use disorders and their consequences, a societal perspective is usually employed.
This perspective includes the overall costs to society, incorporating multiple perspectives such as those of an individual, the government, and the healthcare system. Previous studies that have measured the economic burden of the opioid crisis using a societal perspective typically use a “human capital” approach. This approach typically accounts for healthcare costs, criminal justice costs, and lost productivity, including the loss of wages from premature fatalities. In this study, researchers use the ‘value of a statistical life’ instead of the ‘human capital’ approach to measure morbidity and mortality, substantially increasing the economic burden estimates of opioid use disorder and fatal opioid overdoses compared with previous studies. This method was first used by the Council of Economic Advisors and recognizes that premature fatalities have value beyond their more direct economic impact. Accounting for premature fatalities, using the value of a statistical life, and reduced quality of life from opioid use disorder using the value of a statistical life year, may give a more accurate representation of the total societal welfare loss due to the opioid crisis and better-inform efforts to prevent opioid use disorder and reduce the rate of fatal opioid overdoses.
HOW WAS THIS STUDY CONDUCTED?
This economic analysis used a societal perspective to estimate the nonfatal and fatal costs of the opioid crisis in 2017, with specific measurements for healthcare, criminal justice, and lost productivity. The cost of morbidity resulting from reduced quality of life was measured by the value of a statistical life year ($517,324), and the cost of premature mortality resulting from fatal overdose death was measured by the value of a statistical life ($10.1 million). See below for more detail on how each of these economic impacts were calculated.
Researchers obtained the incidence of fatal opioid overdoses through the National Vital Statistics System and the prevalence of opioid use disorder from the National Survey on Drug Use and Health. According to these data sources, there were 47,600 opioid overdose deaths and 2.13 million people with opioid use disorder in the United States in 2017. Guidelines from the United States Department of Health and Human Services were used to measure morbidity and mortality using the ‘value of a statistical life’ approach. Economic costs were measured in the following categories:
Healthcare: Researchers used a methodology from a previous study to measure the impact of opioid use disorder diagnoses on healthcare spending. This previous study used a claims database to estimate the increased annual healthcare costs associated with opioid use disorder for commercial, Medicaid, and Medicare beneficiaries. The increased costs for each type of insurance beneficiary was then multiplied by the number of people with opioid use disorder derived from the National Survey on Drug Use and Health for each insurance coverage category. To account for opioid use disorder treatment that is not funded by health insurance, federal, state, local, and private expenditures on substance use disorder treatment were identified through SAMHSA. This total was multiplied by the ratio of cases of opioid use disorder among all those with substance use disorder derived from the 2017 National Survey on Drug Use and Health.
Criminal Justice: Researchers divided these costs up by police protection, legal and adjudication, correctional facilities, and property lost due to crimes. The total costs for police protection and legal and adjudication was multiplied by the percentage that was drug related. Then, this figure was multiplied by the ratio of cases of opioid use disorder among all those with a drug use disorder (which included all types of substance use disorders other than alcohol) derived from the 2017 National Survey on Drug Use and Health. The total cost for correctional facilities was calculated by multiplying the cost for those incarcerated with drug-related crimes by the ratio of cases of opioid use disorder among all those with a drug use disorder. Property lost due to crimes was derived from total drug-related property loss multiplied by the ratio of cases of opioid use disorder among all those with a drug use disorder.
Lost Productivity: Researchers used a methodology from a previous study extending to both illicit and prescription opioids. Lost productivity comes from three sources: reduced productive hours from opioid use disorder, incarceration related to opioids, and premature death from opioid overdose. For lost productivity from opioid use disorder, the percentage reduction in productivity attributable to this disorder (17% for males and 18% for females) was multiplied by the average annual production value of the U.S. population and the national prevalence of opioid use disorder from National Survey on Drug Use and Health, taking into account age and gender. For lost productivity from incarceration, the number of those incarcerated for crimes attributable to opioid use disorder were multiplied by the average annual production value of the U.S. population. For premature death from opioid overdose, the value of lost salary and fringe benefits as well as the loss of household production were estimated in a cost module from the CDC.
Valuation of Lost Quality of Life: First, the difference between the health-related quality of life for a person with and without opioid use disorder was calculated using the findings of a previous study. This difference varied based on if a person was an injection drug user, had a prescription opioid use disorder, or had recently initiated treatment. To measure the total valuation due to reduced quality of life, the prevalence of those with opioid use disorder from the National Survey on Drug Use and Health that met each of these categories was multiplied by the reduction in health-related quality of life and then by the value of a statistical life year ($517,324). Valuation of lost quality of life represents a measure of the morbidity of opioid use disorder.
Values of Life Lost: The value of a statistical life ($10.1 million) was multiplied by the number of opioid overdose deaths in 2017 to calculate the value of life lost. Value of life lost represents a measure of the mortality from opioid use disorder, opioid misuse, and opioid use.
The cost in each of these five categories was added together for the total valuation of economic burden of opioid use disorder and fatal overdose. This total valuation was also broken down into nonfatal and fatal costs.
Figure 1.
Previous literature has suggested that opioid use disorder prevalence is underestimated and opioid overdoses as a share of all drug overdose deaths is undercounted. In addition, it is recommended that the value of a statistical life method should provide a low-end and high-end cost. This study also uses data from a variety of sources. Given these variations, the researchers conducted sensitivity analyses using alternative assumptions to test the robustness of their results.
WHAT DID THIS STUDY FIND?
The overall estimated cost of the opioid crisis in 2017 was $1.02 trillion.
A slightly lower amount of this economic burden was attributable to costs related to opioid-related harms ($471 billion) when compared to costs related to opioid-involved deaths ($550 billion).
Most of the costs are from morbidity and mortality.
Over 85% of the total economic burden was from the value of the reduced quality of life from opioid use disorder ($391 billion) and the value of life lost to opioid overdose ($481 billion).
Lost productivity costs were higher than healthcare and criminal justice costs.
Total lost productivity costs amounted to $100 billion and included the nonfatal costs of $23.5 billion due to reduced productivity from opioid use disorder and $7.8 billion due to lost productivity from incarceration, as well as the fatal costs of $68.7 billion due to forgone wages from premature fatality. The cost to healthcare was $34.8 billion, which included $12.9 to private insurance, $11.1 to Medicaid, $3.2 billion to Medicare, and $3.5 billion from funding outside of health insurance. Criminal justice costs amounted to $14.8 billion, with police protection ($6.2 billion) and correctional facilities ($5.4 billion) bearing the largest burden.
Figure 2. Full breakdown of total economic burden in this analysis.
Sensitivity analyses place the economic burden as low as $500 billion and as high as $1.5 trillion.
When different valuations or weights were considered and different assumptions were made about opioid use disorder prevalence and the number of opioid overdose deaths, estimates ranged between $500 billion and $1.5 trillion. The largest fluctuations were seen when using alternative values (low-end and high-end estimates) for a statistical life and alternative weights for health-related quality of life.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that the overall estimated cost of opioid use disorder and fatal opioid overdoses was $1.02 trillion in 2017, with 85% of this burden from the value of the reduced quality of life from opioid use disorder and life lost to opioid overdose, while lost productivity was estimated at $100 billion, healthcare costs were estimated at $34.8 billion, and criminal justice costs estimated at $14.8 billion.
These findings suggest that a substantial amount of value in the U.S. economy is lost due to the opioid crisis, highlighting that considerable economic benefits can be reaped from a two-pronged approach of preventing opioid use disorder and reducing the rate of fatal opioid overdoses. In fact, a recent study using a similar methodology estimates that preventing one case of opioid use disorder would save society $2.2 million. Strategies to prevent opioid use disorder include interventions and policies to promote cautious prescribing of opioids such as prescription drug monitoring programs and state prescription drug laws, safe storage and disposal of prescription opioids, and early interventionof prescription opioid misuse. Also, primary prevention of opioid misuse may be part of evidence-based prevention in children and teens that targets enhanced social and developmental skills.
In addition to preventing opioid use disorder, there are several treatment and harm reduction strategies that have been shown to reduce opioid overdose deaths, lessening the economic burden of the opioid crisis. Medications for opioid use disorder, especially opioid agonists such as methadone and buprenorphine, have been shown to reduce overdose mortality for those with an opioid use disorder. Emerging evidence suggests that initiation of these medications in certain settings, such as emergency departmentsand the criminal justice system, have the potential to reduce mortality substantially. Other promising models for initiation include post-overdose response teams and peer outreach. In addition to initiation, strategies for retaining individuals on medications for opioid use disorder are crucial to improve long-term outcomes. High-risk individuals and their family members should have access to naloxone, an opioid overdose antidote, which has been shown to be one of the most effective strategies in reducing opioid overdose mortality. Given the human and economic toll of the opioid crisis, more innovative yet controversial approaches might be considered, including drug checking services, safe consumption sites, and safe drug supply.
Although the reduction in quality of life from opioid use disorder and life lost to opioid overdose, as measured by the value of a statistical life, made up the large majority of the economic costs attributable to the opioid crisis, lost productivity ($100 billion), increased healthcare costs ($34.8 billion), and increased criminal justice costs ($14.8 billion) were sizeable. Lost productivity may directly affect employers and indirectly affect the government, through lost tax revenues. Employer-led initiatives, such as recovery friendly workplaces, hold promise. Stakeholders in the healthcare system and the criminal justice system may benefit from implementing many of the strategies already discussed to prevent opioid use disorder and reduce overdose mortality.
Some of the creative efforts to capture all costs associated with an illness can become more of an art than a science. This is especially true regarding the new methodology employed by this study to measure premature fatalities and reduced quality of life using the value of a statistical life.
Previous studies have primarily used a ‘human capital’ approach, which totals the economic loss of a premature fatality by measuring lost economic output. The ‘value of a statistical life’ approach is typically used in policy analyses as a willingness-to-pay for risk reduction by individuals or society.
Used in a cost-of-illness analysis, the ‘value of a statistical life’ approach will result in a much higher total economic cost than the ‘human capital’ approach. However, the true economic toll of reduced quality of life and premature fatality from the opioid crisis is likely to fall somewhere between these two approaches.
Given that measuring the societal economic burden of substance-related harms has historically used a ‘human capital’ approach, the ‘value of a statistical life’ approach could serve as a model for understanding the ‘true’ costs of other substances, especially alcohol, which carries the largest public health burden because of its wide availability, normalized use, toxicity, and the presence of a profit-maximizing industry that markets its use. More research is needed to determine which methodology more accurately captures the overall economic burden of the opioid crisis and how this methodology might translate to other substances.
Typically, cost-of-illness studies use a ‘human capital’ approach in measuring the economic valuation of morbidity and mortality. Adding the value of a statistical life to measure valuation beyond economic output, which accounts for 85% of the total burden in this study, may overestimate the actual economic impact of the opioid crisis possibly leading to some stakeholders discrediting economic cost burden analyses.
The ratio of opioid use disorder cases among those with a substance use disorder or drug use disorder (all substance use disorders except alcohol) was used for many of the calculations. However, certain types of substances may disproportionately affect costs. For instance, criminal justice costs may be higher on average for people with opioid use disorder compared to people with a cannabis use disorder, both considered types of drug use disorders.
This study uses averages across the entire United States population which may not be representative of the population with opioid use disorder. For example, the societal willingness to pay, or the value of a statistical life, may be different for preventing a fatal opioid overdose than the general value used in this study. Also, the average earnings of the U.S. population may not be representative of the earnings for those with opioid use disorder.
There is uncertainty in the national prevalence of opioid use disorder and the share of opioid overdose deaths among all drug overdose deaths. Though a higher share of opioid overdose deaths is accounted for in sensitivity analyses, the study does not examine the likely scenario that national opioid use disorder prevalence is twofold or more higher than that reported by the National Survey on Drug Use and Health.
Some ripple effects of the opioid crisis are not captured in this economic analysis, such as the healthcare costs of neonatal abstinence syndrome and the reduced quality of life experienced by family members of those with opioid use disorder.
Most opioid overdose deaths have an additional non-opioid substance present on the toxicology report and most people with opioid use disorder use multiple substances. Therefore, it is difficult to attribute the economic costs in this study entirely to opioids.
This study appears to take a ‘value of a statistical life’ approach to measuring the economic loss of premature fatality rather than a ‘human capital’ approach. However, lost productivity is included as a fatal cost in the economic analysis, likely double counting the economic loss due to premature fatality.
BOTTOM LINE
This study found that the overall estimated cost of opioid use disorder and fatal opioid overdoses was $1.02 trillion in 2017, with 85% of this burden from the value of the reduced quality of life from opioid use disorder and life lost to opioid overdose, while lost productivity was estimated at $100 billion, healthcare costs were estimated at $34.8 billion, and criminal justice costs estimated at $14.8 billion.
For individuals and families seeking recovery: In addition to the human toll, the opioid crisis has a substantial economic impact. Safe storage and disposal of prescription opioids is one way to prevent prescription opioid misuse and opioid use disorder. Medications for opioid use disorder, such as buprenorphine, methadone, and extended-release naltrexone, have been shown to be effective treatment options. Individuals at high-risk for opioid overdose and their families also should have access to naloxone in case of emergency.
For treatment professionals and treatment systems: There are substantial economic benefits from implementing evidence-based interventions that prevent opioid use disorder and reduce opioid overdose deaths, in addition to improving clinical outcomes. Some of these interventions may include early intervention for prescription opioid misuse, having the capacity to provide medications for opioid use disorder when indicated, distributing naloxone to high-risk individuals, and linkage to local harm reduction services such as syringe service programs.
For scientists:This cost-of-illness study uses a new methodology to assess reduced quality of life and premature fatality, the value of a statistical life, which goes beyond measuring an individual’s economic output. This methodology would benefit from future research to examine if a measure typically used in policy analyses as a willingness-to-pay for risk reduction is more accurate in capturing overall economic costs in a cost-of-illness study compared with the human capital approach. The findings of this study show that there are substantial economic benefits of preventing opioid use disorder and reducing opioid overdose deaths, highlighting the need for evaluating policies and interventions based on these outcomes.
For policy makers: There are substantial economic benefits to be reaped from implementing evidence-based interventions and policies that prevent opioid use disorder and reduce opioid overdose deaths. Interventions to ensure cautious opioid prescribing, such as prescription drug monitoring programs, academic detailing, and state prescription drug laws, can prevent the onset of new cases of opioid use disorder. Emerging evidence suggests that policies to expand the availability of medications for opioid use disorder and naloxone in high-risk settings, such as emergency departments and the criminal justice system, can reduce opioid overdose deaths. Given the human and economic toll of the opioid crisis, more innovative approaches that are utilized in other industrialized nations but have proved more controversial in the United States might be considered, including drug checking services, safe consumption sites, and safe drug supply.
The opioid crisis has claimed nearly 450,000 lives in the last 20 years, with recent evidence showing that overdose deaths reached an all-time highin 2019 and preliminary evidence suggesting that the coronavirus pandemic has further exacerbated these deaths. Understanding the overall economic impact of the opioid crisis is crucial in drawing public attention to it, increasing political will, and in mobilizing and investing in necessary resources to address it and curb costs. In addition, decision-makers need to know how specific parts of the economy are affected by opioid-related harms. For example, employers will be interested in how the productivity of their workers is affected whereas criminal justice stakeholders might be interested in the cost to correctional facilities.
Economic cost analyses assume different stakeholder perspectives (e.g., taxpayer, government, health insurer) when estimating overall costs. In a cost-of-illness study, such as one that comprehensively measures the economic impact of opioid use disorders and their consequences, a societal perspective is usually employed.
This perspective includes the overall costs to society, incorporating multiple perspectives such as those of an individual, the government, and the healthcare system. Previous studies that have measured the economic burden of the opioid crisis using a societal perspective typically use a “human capital” approach. This approach typically accounts for healthcare costs, criminal justice costs, and lost productivity, including the loss of wages from premature fatalities. In this study, researchers use the ‘value of a statistical life’ instead of the ‘human capital’ approach to measure morbidity and mortality, substantially increasing the economic burden estimates of opioid use disorder and fatal opioid overdoses compared with previous studies. This method was first used by the Council of Economic Advisors and recognizes that premature fatalities have value beyond their more direct economic impact. Accounting for premature fatalities, using the value of a statistical life, and reduced quality of life from opioid use disorder using the value of a statistical life year, may give a more accurate representation of the total societal welfare loss due to the opioid crisis and better-inform efforts to prevent opioid use disorder and reduce the rate of fatal opioid overdoses.
HOW WAS THIS STUDY CONDUCTED?
This economic analysis used a societal perspective to estimate the nonfatal and fatal costs of the opioid crisis in 2017, with specific measurements for healthcare, criminal justice, and lost productivity. The cost of morbidity resulting from reduced quality of life was measured by the value of a statistical life year ($517,324), and the cost of premature mortality resulting from fatal overdose death was measured by the value of a statistical life ($10.1 million). See below for more detail on how each of these economic impacts were calculated.
Researchers obtained the incidence of fatal opioid overdoses through the National Vital Statistics System and the prevalence of opioid use disorder from the National Survey on Drug Use and Health. According to these data sources, there were 47,600 opioid overdose deaths and 2.13 million people with opioid use disorder in the United States in 2017. Guidelines from the United States Department of Health and Human Services were used to measure morbidity and mortality using the ‘value of a statistical life’ approach. Economic costs were measured in the following categories:
Healthcare: Researchers used a methodology from a previous study to measure the impact of opioid use disorder diagnoses on healthcare spending. This previous study used a claims database to estimate the increased annual healthcare costs associated with opioid use disorder for commercial, Medicaid, and Medicare beneficiaries. The increased costs for each type of insurance beneficiary was then multiplied by the number of people with opioid use disorder derived from the National Survey on Drug Use and Health for each insurance coverage category. To account for opioid use disorder treatment that is not funded by health insurance, federal, state, local, and private expenditures on substance use disorder treatment were identified through SAMHSA. This total was multiplied by the ratio of cases of opioid use disorder among all those with substance use disorder derived from the 2017 National Survey on Drug Use and Health.
Criminal Justice: Researchers divided these costs up by police protection, legal and adjudication, correctional facilities, and property lost due to crimes. The total costs for police protection and legal and adjudication was multiplied by the percentage that was drug related. Then, this figure was multiplied by the ratio of cases of opioid use disorder among all those with a drug use disorder (which included all types of substance use disorders other than alcohol) derived from the 2017 National Survey on Drug Use and Health. The total cost for correctional facilities was calculated by multiplying the cost for those incarcerated with drug-related crimes by the ratio of cases of opioid use disorder among all those with a drug use disorder. Property lost due to crimes was derived from total drug-related property loss multiplied by the ratio of cases of opioid use disorder among all those with a drug use disorder.
Lost Productivity: Researchers used a methodology from a previous study extending to both illicit and prescription opioids. Lost productivity comes from three sources: reduced productive hours from opioid use disorder, incarceration related to opioids, and premature death from opioid overdose. For lost productivity from opioid use disorder, the percentage reduction in productivity attributable to this disorder (17% for males and 18% for females) was multiplied by the average annual production value of the U.S. population and the national prevalence of opioid use disorder from National Survey on Drug Use and Health, taking into account age and gender. For lost productivity from incarceration, the number of those incarcerated for crimes attributable to opioid use disorder were multiplied by the average annual production value of the U.S. population. For premature death from opioid overdose, the value of lost salary and fringe benefits as well as the loss of household production were estimated in a cost module from the CDC.
Valuation of Lost Quality of Life: First, the difference between the health-related quality of life for a person with and without opioid use disorder was calculated using the findings of a previous study. This difference varied based on if a person was an injection drug user, had a prescription opioid use disorder, or had recently initiated treatment. To measure the total valuation due to reduced quality of life, the prevalence of those with opioid use disorder from the National Survey on Drug Use and Health that met each of these categories was multiplied by the reduction in health-related quality of life and then by the value of a statistical life year ($517,324). Valuation of lost quality of life represents a measure of the morbidity of opioid use disorder.
Values of Life Lost: The value of a statistical life ($10.1 million) was multiplied by the number of opioid overdose deaths in 2017 to calculate the value of life lost. Value of life lost represents a measure of the mortality from opioid use disorder, opioid misuse, and opioid use.
The cost in each of these five categories was added together for the total valuation of economic burden of opioid use disorder and fatal overdose. This total valuation was also broken down into nonfatal and fatal costs.
Figure 1.
Previous literature has suggested that opioid use disorder prevalence is underestimated and opioid overdoses as a share of all drug overdose deaths is undercounted. In addition, it is recommended that the value of a statistical life method should provide a low-end and high-end cost. This study also uses data from a variety of sources. Given these variations, the researchers conducted sensitivity analyses using alternative assumptions to test the robustness of their results.
WHAT DID THIS STUDY FIND?
The overall estimated cost of the opioid crisis in 2017 was $1.02 trillion.
A slightly lower amount of this economic burden was attributable to costs related to opioid-related harms ($471 billion) when compared to costs related to opioid-involved deaths ($550 billion).
Most of the costs are from morbidity and mortality.
Over 85% of the total economic burden was from the value of the reduced quality of life from opioid use disorder ($391 billion) and the value of life lost to opioid overdose ($481 billion).
Lost productivity costs were higher than healthcare and criminal justice costs.
Total lost productivity costs amounted to $100 billion and included the nonfatal costs of $23.5 billion due to reduced productivity from opioid use disorder and $7.8 billion due to lost productivity from incarceration, as well as the fatal costs of $68.7 billion due to forgone wages from premature fatality. The cost to healthcare was $34.8 billion, which included $12.9 to private insurance, $11.1 to Medicaid, $3.2 billion to Medicare, and $3.5 billion from funding outside of health insurance. Criminal justice costs amounted to $14.8 billion, with police protection ($6.2 billion) and correctional facilities ($5.4 billion) bearing the largest burden.
Figure 2. Full breakdown of total economic burden in this analysis.
Sensitivity analyses place the economic burden as low as $500 billion and as high as $1.5 trillion.
When different valuations or weights were considered and different assumptions were made about opioid use disorder prevalence and the number of opioid overdose deaths, estimates ranged between $500 billion and $1.5 trillion. The largest fluctuations were seen when using alternative values (low-end and high-end estimates) for a statistical life and alternative weights for health-related quality of life.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that the overall estimated cost of opioid use disorder and fatal opioid overdoses was $1.02 trillion in 2017, with 85% of this burden from the value of the reduced quality of life from opioid use disorder and life lost to opioid overdose, while lost productivity was estimated at $100 billion, healthcare costs were estimated at $34.8 billion, and criminal justice costs estimated at $14.8 billion.
These findings suggest that a substantial amount of value in the U.S. economy is lost due to the opioid crisis, highlighting that considerable economic benefits can be reaped from a two-pronged approach of preventing opioid use disorder and reducing the rate of fatal opioid overdoses. In fact, a recent study using a similar methodology estimates that preventing one case of opioid use disorder would save society $2.2 million. Strategies to prevent opioid use disorder include interventions and policies to promote cautious prescribing of opioids such as prescription drug monitoring programs and state prescription drug laws, safe storage and disposal of prescription opioids, and early interventionof prescription opioid misuse. Also, primary prevention of opioid misuse may be part of evidence-based prevention in children and teens that targets enhanced social and developmental skills.
In addition to preventing opioid use disorder, there are several treatment and harm reduction strategies that have been shown to reduce opioid overdose deaths, lessening the economic burden of the opioid crisis. Medications for opioid use disorder, especially opioid agonists such as methadone and buprenorphine, have been shown to reduce overdose mortality for those with an opioid use disorder. Emerging evidence suggests that initiation of these medications in certain settings, such as emergency departmentsand the criminal justice system, have the potential to reduce mortality substantially. Other promising models for initiation include post-overdose response teams and peer outreach. In addition to initiation, strategies for retaining individuals on medications for opioid use disorder are crucial to improve long-term outcomes. High-risk individuals and their family members should have access to naloxone, an opioid overdose antidote, which has been shown to be one of the most effective strategies in reducing opioid overdose mortality. Given the human and economic toll of the opioid crisis, more innovative yet controversial approaches might be considered, including drug checking services, safe consumption sites, and safe drug supply.
Although the reduction in quality of life from opioid use disorder and life lost to opioid overdose, as measured by the value of a statistical life, made up the large majority of the economic costs attributable to the opioid crisis, lost productivity ($100 billion), increased healthcare costs ($34.8 billion), and increased criminal justice costs ($14.8 billion) were sizeable. Lost productivity may directly affect employers and indirectly affect the government, through lost tax revenues. Employer-led initiatives, such as recovery friendly workplaces, hold promise. Stakeholders in the healthcare system and the criminal justice system may benefit from implementing many of the strategies already discussed to prevent opioid use disorder and reduce overdose mortality.
Some of the creative efforts to capture all costs associated with an illness can become more of an art than a science. This is especially true regarding the new methodology employed by this study to measure premature fatalities and reduced quality of life using the value of a statistical life.
Previous studies have primarily used a ‘human capital’ approach, which totals the economic loss of a premature fatality by measuring lost economic output. The ‘value of a statistical life’ approach is typically used in policy analyses as a willingness-to-pay for risk reduction by individuals or society.
Used in a cost-of-illness analysis, the ‘value of a statistical life’ approach will result in a much higher total economic cost than the ‘human capital’ approach. However, the true economic toll of reduced quality of life and premature fatality from the opioid crisis is likely to fall somewhere between these two approaches.
Given that measuring the societal economic burden of substance-related harms has historically used a ‘human capital’ approach, the ‘value of a statistical life’ approach could serve as a model for understanding the ‘true’ costs of other substances, especially alcohol, which carries the largest public health burden because of its wide availability, normalized use, toxicity, and the presence of a profit-maximizing industry that markets its use. More research is needed to determine which methodology more accurately captures the overall economic burden of the opioid crisis and how this methodology might translate to other substances.
Typically, cost-of-illness studies use a ‘human capital’ approach in measuring the economic valuation of morbidity and mortality. Adding the value of a statistical life to measure valuation beyond economic output, which accounts for 85% of the total burden in this study, may overestimate the actual economic impact of the opioid crisis possibly leading to some stakeholders discrediting economic cost burden analyses.
The ratio of opioid use disorder cases among those with a substance use disorder or drug use disorder (all substance use disorders except alcohol) was used for many of the calculations. However, certain types of substances may disproportionately affect costs. For instance, criminal justice costs may be higher on average for people with opioid use disorder compared to people with a cannabis use disorder, both considered types of drug use disorders.
This study uses averages across the entire United States population which may not be representative of the population with opioid use disorder. For example, the societal willingness to pay, or the value of a statistical life, may be different for preventing a fatal opioid overdose than the general value used in this study. Also, the average earnings of the U.S. population may not be representative of the earnings for those with opioid use disorder.
There is uncertainty in the national prevalence of opioid use disorder and the share of opioid overdose deaths among all drug overdose deaths. Though a higher share of opioid overdose deaths is accounted for in sensitivity analyses, the study does not examine the likely scenario that national opioid use disorder prevalence is twofold or more higher than that reported by the National Survey on Drug Use and Health.
Some ripple effects of the opioid crisis are not captured in this economic analysis, such as the healthcare costs of neonatal abstinence syndrome and the reduced quality of life experienced by family members of those with opioid use disorder.
Most opioid overdose deaths have an additional non-opioid substance present on the toxicology report and most people with opioid use disorder use multiple substances. Therefore, it is difficult to attribute the economic costs in this study entirely to opioids.
This study appears to take a ‘value of a statistical life’ approach to measuring the economic loss of premature fatality rather than a ‘human capital’ approach. However, lost productivity is included as a fatal cost in the economic analysis, likely double counting the economic loss due to premature fatality.
BOTTOM LINE
This study found that the overall estimated cost of opioid use disorder and fatal opioid overdoses was $1.02 trillion in 2017, with 85% of this burden from the value of the reduced quality of life from opioid use disorder and life lost to opioid overdose, while lost productivity was estimated at $100 billion, healthcare costs were estimated at $34.8 billion, and criminal justice costs estimated at $14.8 billion.
For individuals and families seeking recovery: In addition to the human toll, the opioid crisis has a substantial economic impact. Safe storage and disposal of prescription opioids is one way to prevent prescription opioid misuse and opioid use disorder. Medications for opioid use disorder, such as buprenorphine, methadone, and extended-release naltrexone, have been shown to be effective treatment options. Individuals at high-risk for opioid overdose and their families also should have access to naloxone in case of emergency.
For treatment professionals and treatment systems: There are substantial economic benefits from implementing evidence-based interventions that prevent opioid use disorder and reduce opioid overdose deaths, in addition to improving clinical outcomes. Some of these interventions may include early intervention for prescription opioid misuse, having the capacity to provide medications for opioid use disorder when indicated, distributing naloxone to high-risk individuals, and linkage to local harm reduction services such as syringe service programs.
For scientists:This cost-of-illness study uses a new methodology to assess reduced quality of life and premature fatality, the value of a statistical life, which goes beyond measuring an individual’s economic output. This methodology would benefit from future research to examine if a measure typically used in policy analyses as a willingness-to-pay for risk reduction is more accurate in capturing overall economic costs in a cost-of-illness study compared with the human capital approach. The findings of this study show that there are substantial economic benefits of preventing opioid use disorder and reducing opioid overdose deaths, highlighting the need for evaluating policies and interventions based on these outcomes.
For policy makers: There are substantial economic benefits to be reaped from implementing evidence-based interventions and policies that prevent opioid use disorder and reduce opioid overdose deaths. Interventions to ensure cautious opioid prescribing, such as prescription drug monitoring programs, academic detailing, and state prescription drug laws, can prevent the onset of new cases of opioid use disorder. Emerging evidence suggests that policies to expand the availability of medications for opioid use disorder and naloxone in high-risk settings, such as emergency departments and the criminal justice system, can reduce opioid overdose deaths. Given the human and economic toll of the opioid crisis, more innovative approaches that are utilized in other industrialized nations but have proved more controversial in the United States might be considered, including drug checking services, safe consumption sites, and safe drug supply.