Staff experiences with a legislative mandate to provide buprenorphine and methadone in correctional settings
Individuals with opioid use disorder who have been incarcerated are at increased risk for overdose upon release. Providing medications during incarceration can help reduce this risk, but few correctional facilities currently offer them. This study examined the implementation of a state legislative mandate to provide access to methadone and buprenorphine in jails.
Individuals with opioid use disorder who have been incarcerated are at an increased risk for overdose and death upon release. This is because abstinence during incarceration leads to decreased tolerance. Then, if individuals begin to use again upon release at the same level they did before incarceration, their risk for overdose is greatly increased.
Medications for opioid use disorder that are administered during incarceration can be helpful in preventing overdoses upon release, as well as leading to treatment entry and reducing risky behaviors, such as syringe sharing, which can increase risk of infectious disease transmission. However, while some jails and prisons are beginning to offer medications for opioid use disorder, it is still not a routine practice. This may be due to logistical barriers, such as the need for licensed medical staff and expenses. Of note, the administration of opioid agonist medications, such as methadone and buprenorphine, is subject to specific state and federal regulations that antagonist medications (e.g., naltrexone) are not. For instance, methadone must be administered in a licensed facility and, until recently, buprenorphine must be prescribed by a physician with specialized training. These regulations likely make medication administration in jail settings difficult.
In 2018, Massachusetts became the first state in the US to pass a legislative mandate to pilot the provision of access to medications for opioid use disorder in jails. This mandate states that medications must be maintained in individuals who were receiving it before being detained and initiated among those who may need it. It also states that jails must facilitate continuation of medications after detainees are released.
Any number of factors may either facilitate or hinder the implementation of such a mandate, including leadership and staffing within the jail and collaborations with community-based organizations. In this study, the research team interviewed jail staff and held focus groups to learn about the facilitators and barriers to implementing the mandate in Massachusetts during the first year. Understanding what is needed to effectively implement medications for opioid use disorder in jails and link individuals to treatment upon release can help inform new policies and programming, thereby ultimately reducing risk for overdose and death.
HOW WAS THIS STUDY CONDUCTED?
The research team interviewed and held focus groups with jail staff about their perspectives regarding the first year of implementing the state legislative mandate in Massachusetts to provide access to medications for opioid use disorders in jails. The research was conducted across 7 Massachusetts county jails that had complied with the legislative mandate to expand access to medications approved by the Food and Drug Administration (FDA) to treat opioid use disorder. In particular, access to buprenorphine and methadone was expanded, given that these facilities were already providing access to naltrexone.
The research team conducted interviews and focus groups. Senior jail staff were interviewed individually, and other staff participated in the focus groups, which ranged in size from 2-11 participants. Interviews and focus groups were recorded so they could later be transcribed and coded for themes that emerged from participants’ responses. The research team coded the responses using standard qualitative methods and categories.
Outcomes of interest include internal and external contextual factors that influenced implementation of the mandate. External, or outer, factors included service environment, funding, and characteristics of the service recipients, while internal, or inner, factors included organizational characteristics and leadership, fidelity monitoring, and staff perspectives and hiring practices. Bridging factors were also examined, which included relationships between and within organizations, as well as relationships with community providers.
Participants included 61 clinical, corrections, and senior administrative staff who were recommended by jail administrators because of their involvement with decision-making regarding implementation of the policy. Most identified as White (80.3%) and as female (60.7%), with a mean age of 45 and a master’s degree level of education (45.9%). Many of the participants’ jobs involved behavioral health or addiction treatment (38.6%) or were administrative (29.8%). Among these, 27.3% had been working in their current position for less than 1 year, 25.5% had been for 1-3 years, and 32.7% had been for 4-9 years. Only 12.7% had been in their current position for more than 10 years. However, many of the participants had been working in their current agency for more than 10 years (41.8%) or 4-9 years (36.4%).
WHAT DID THIS STUDY FIND?
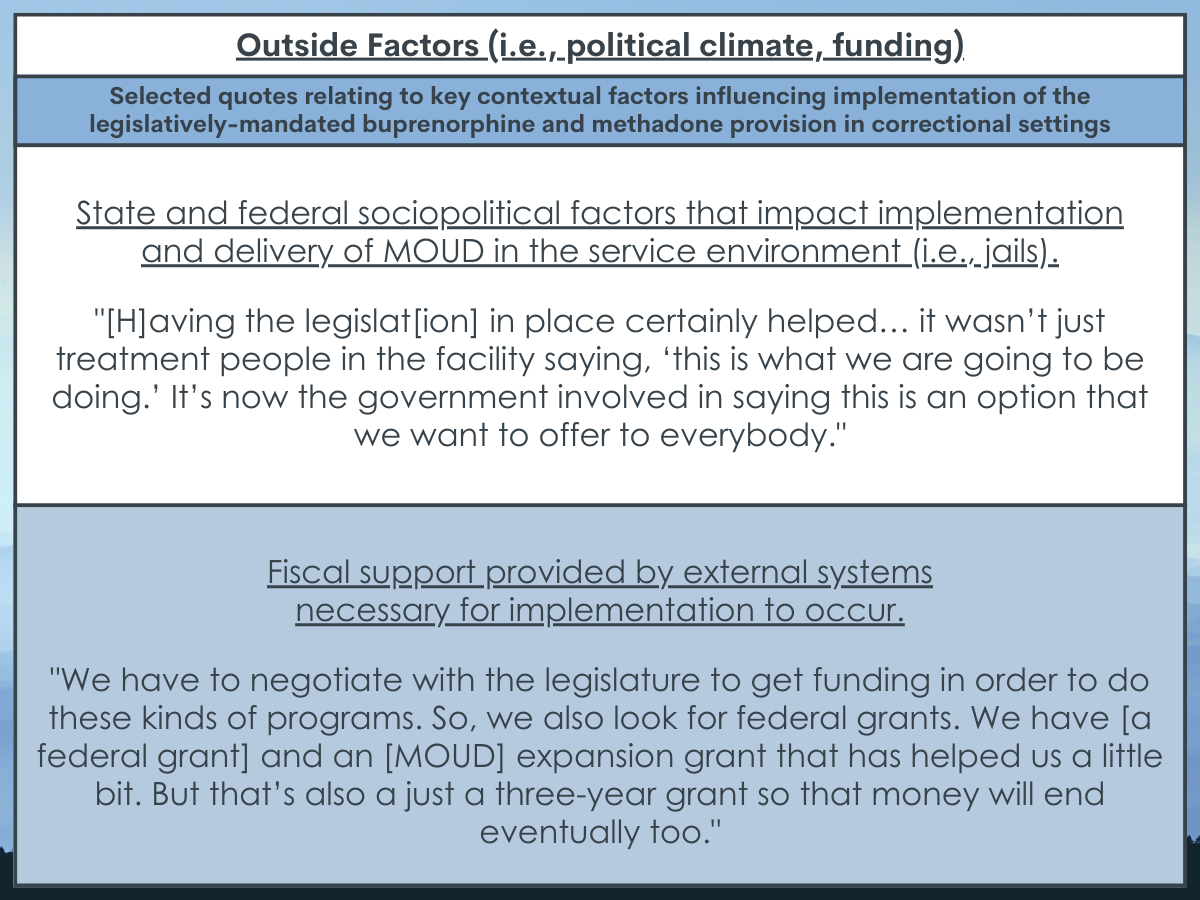
The broader political climate and funding helped facilitate implementation.
Implementation occurred during national and statewide shifts towards greater acceptance of treating opioid use disorder with medications. These shifts are evident by the mandate and by the state court’s ruling that failure to provide methadone violated constitutional rights, which occurred during the same time. Participants described how these broader shifts helped lead to acceptance among jail staff, particularly among newer and younger staff, and a “culture shift” from viewing medication treatment as illicit to necessary.
Participants also discussed how funding provided by the mandate was helpful for administering the medications and ensuring medication treatment would be continued after release.
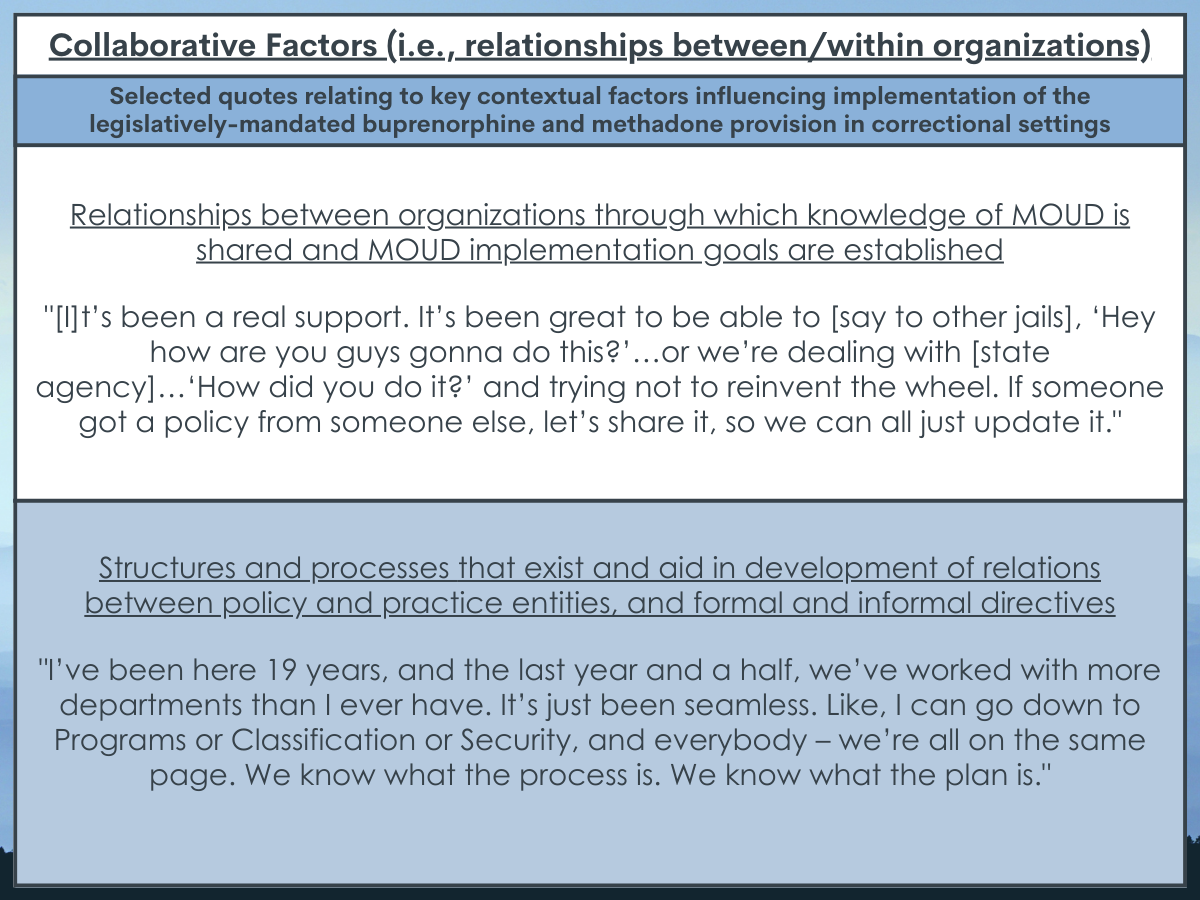
Collaborations within and between organizations improved problem solving and efficiency.
Participants described how implementation helped to build collaborations between disciplines within the organization, which led to a more “cohesive” jail and the ability to develop solutions to problems. Likewise, collaborating with community-based organizations that they had established and trusting relationships with helped them solve problems and reduced the burden of developing new contracts and training new staff to implement the mandate.
Most participants said that collaboration with the state agency overseeing implementation was important to develop trust and identify practical limitations. However, some staff mentioned that they felt that the state agency did not sufficiently consider their perspectives.
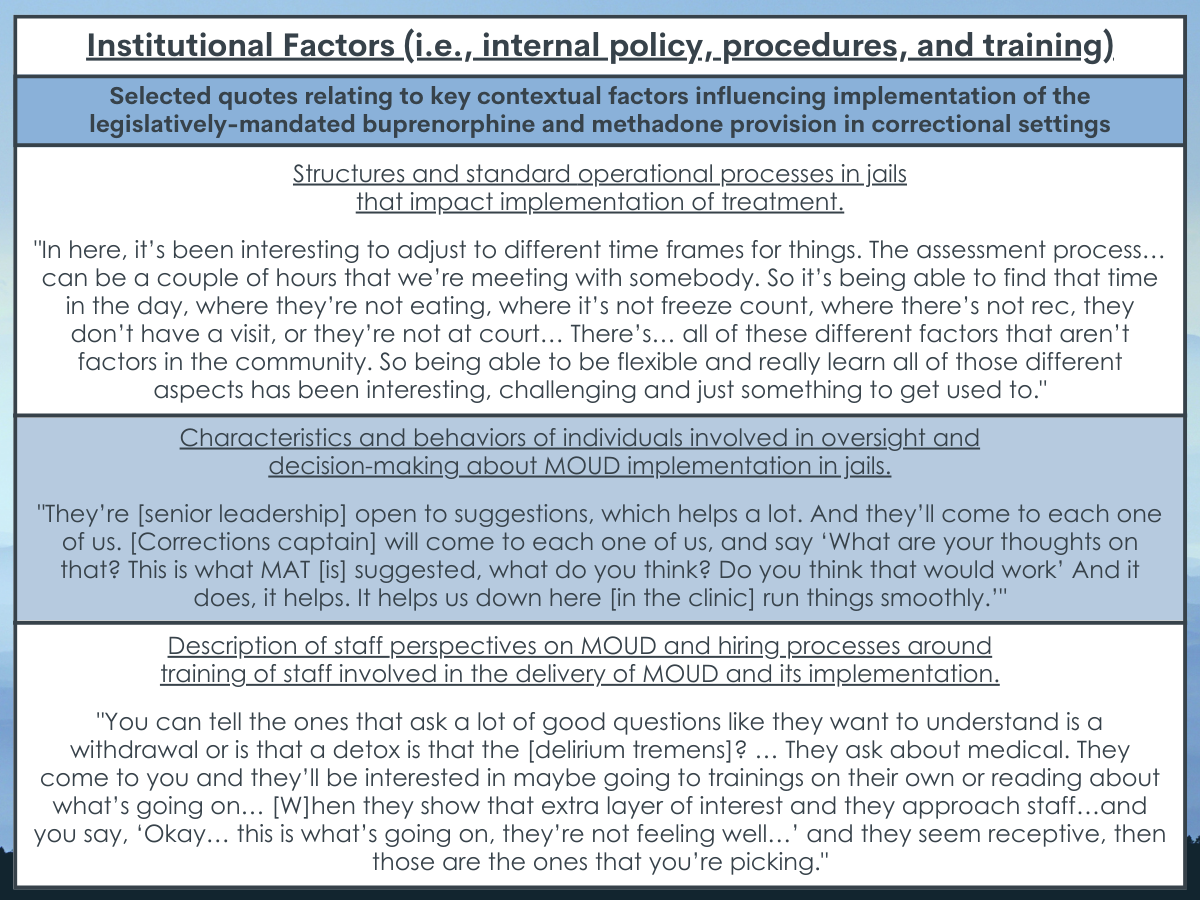
Institutional policies, procedures, and training improve implementation.
Participants discussed the need for institutional policy and procedures to implement the mandate, with a key challenge being the determination of how to and who would administer medications. For instance, an important decision point was whether to develop an onsite treatment program or transport people offsite. This is because certain medications, such as methadone and buprenorphine, are subject to specific state and federal regulations (e.g., methadone be administered in a licensed facility; buprenorphine must be prescribed by a physician with specialized training).
Further, although many staff were accepting of the program, some staff, like medical staff, were concerned about “substituting one addiction for another.” However, participants discussed how this was alleviated with training and the fact that it was offered along with psychosocial therapy. Younger staff also tended to be more accepting of the program, which may be because they grew up during the opioid overdose epidemic and were most impacted. The growing shift towards a public health approach to addiction, as opposed to punitive approaches, that they grew up with also likely influenced their openness to agonist medications.
Finally, participants described how important it was for organizational leadership to listen to, and incorporate, feedback from staff. Leaders discussed how they worked to break down traditional power hierarchies and silos to encourage open communication about implementation and guide adaptations of existing procedures as needed.
Additional challenges with implementation were highlighted.
Participants discussed how confusion around sentencing and release dates made coordinating continuation of care challenging. Specifically,the main issues included not knowing whether pre-trial individuals would be sentenced, and if sentenced, not knowing people’s release dates,as well asnot knowing who might end up in a facility without access to medications. In addition, the burdensome and redundant nature of the reporting requirements was a challenge, but staff recognized the importance of it.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study interviewed jail staff to understand their perspectives regarding barriers and facilitators of the state legislative mandate in Massachusetts to provide access to medications for opioid use disorders in jails. Staff participants highlighted key facilitators of implementation involving the broader political climate, funding, and collaborations within and between organizations. A number of barriers and challenges were also highlighted, however, including the need for policies and procedures regarding how to and who will administer medications, the importance of staff training and education, and the importance of flexibility from leadership to adapt existing procedures according to staff feedback. Uncertainty around sentencing and release dates, as well as burdensome reporting requirements, were mentioned as additional challenges with implementation.
These findings are consistent with similar research conducted around the same time, but with correctional facilities across the US that were voluntarily providing access to medication for opioid use disorder. Notably, both sets of results, along with additional research, highlighted the challenges of adhering to state and federal regulations regarding agonist medication administration, the crucial importance of leadership and collaboration, and the growing culture shifts towards greater acceptance of medication treatment. An important difference, however, was that participants from facilities that offered medications voluntarily mentioned a lack of funding as a key barrier, while participants from facilities in Massachusetts that were mandated to offer medications discussed how funding was a key facilitator. This underscores the need for policies that allocate adequate funds for implementation.
Results from this study add to a growing number of studies providing consensus about what is needed to effectively implement medications for opioid use disorder in jails and link individuals to treatment upon release. Taken together, this research can help inform new policies and programming. For example, the strict regulations regarding administration of methadone may need to be relaxed or adapted for jail settings. Further, while the broader political environment helped to promote acceptance of medication treatment, staff training and education are needed to continue to reduce stigma and grow acceptance. Finally, since implementation requires collaboration with community-based organizations, preparing for implementation may involve a capacity-building phase where opportunities for collaboration are pursued.
Ultimately, understanding these barriers and facilitators can inform policies and programming, which can lead to effective and widespread implementation of providing access to medication for opioid use disorder in jails. This can help address the high-risk period for overdose following release and prevent deaths.
Participants were interviewed about their experiences with implementation during the first year of the mandate. As such, participants responses reflected factors that influenced preparation for and initiation of implementation. Responses from interviews conducted later will likely change to reflect how staff are working to sustain the program and their perspectives on potential outcomes.
Participants were staff who were recommended for recruitment because of their involvement with decision-making regardingimplementation of the policy. Therefore, they may have been biased towards its success and responded accordingly and could only offer insights from their specific viewpoint. Other staff who were not involved in decision-making may have had different perspectives and provided different responses.
There may have also been differences between staff roles and amount of time worked at the organization, but these potential differences were not examined due to the limitations in the study design.
The study took place in a northeast state in the US that had adequate resources and support. Results from the study therefore may not generalize to other states or countries with less resources and support.
BOTTOM LINE
Results from this study highlighted both barriers to and facilitators ofimplementingthe state legislative mandate in Massachusetts to provide access to medications for opioid use disorders in jails. Understanding these factors can inform policies and programming, which can ultimately help address the high-risk period for overdose following release and prevent deaths.
For individuals and families seeking recovery: Medication treatment during incarceration is not yet widely available in correctional settings.However, individuals who have the opportunity to take advantage of medication offerings where available are likely to have a lower risk for overdose upon release and potentially a higher likelihood of entering treatment. If not available during incarceration, however, individuals who begin medication treatment after their release are likely to experience similar benefits.
For treatment professionals and treatment systems: Jail systems that have the goal of implementing access to medications for opioid use disorder, or are in the beginning phases of implementation, can use the findings from this study to help guide them.Providing staff training and education, incorporating staff feedback into the adaptation of existing procedures, and collaborating within and between organizations are all likely to help implementation. If implementation is not feasible, however, jail administrators who provide individuals with opioid use disorder information about the risks of overdose upon release and how to obtain medication treatment may also help to prevent overdoses and deaths.
For scientists: While there have been a number of qualitative studies conducted to understand the barriers and facilitators to implementation of access to medication in jails, quantitative research and additional qualitative research in a variety of states with more limited resources will help us to understand the extent to which these results generalize. Perspectives from staff who were not involved in the decision-making process will also help to provide a more comprehensive understanding of the factors that influenced implementation. Finally, research that examines barriers and facilitators during a later stage of implementation will shed light on the factors that influence sustaining the program and potential outcomes.
For policy makers: Results from this study highlighted two important and actionable recommendations for policy makers. First, relaxing or adapting the strict regulations regarding administration of agonist medications in jail settings can help address this challenge to effective and streamlined implementation. Second, policies that allocate funding for implementation of access to medication in jails can help expand medication treatment programs in jails, thereby reducing risk of overdose and death following release.
Individuals with opioid use disorder who have been incarcerated are at an increased risk for overdose and death upon release. This is because abstinence during incarceration leads to decreased tolerance. Then, if individuals begin to use again upon release at the same level they did before incarceration, their risk for overdose is greatly increased.
Medications for opioid use disorder that are administered during incarceration can be helpful in preventing overdoses upon release, as well as leading to treatment entry and reducing risky behaviors, such as syringe sharing, which can increase risk of infectious disease transmission. However, while some jails and prisons are beginning to offer medications for opioid use disorder, it is still not a routine practice. This may be due to logistical barriers, such as the need for licensed medical staff and expenses. Of note, the administration of opioid agonist medications, such as methadone and buprenorphine, is subject to specific state and federal regulations that antagonist medications (e.g., naltrexone) are not. For instance, methadone must be administered in a licensed facility and, until recently, buprenorphine must be prescribed by a physician with specialized training. These regulations likely make medication administration in jail settings difficult.
In 2018, Massachusetts became the first state in the US to pass a legislative mandate to pilot the provision of access to medications for opioid use disorder in jails. This mandate states that medications must be maintained in individuals who were receiving it before being detained and initiated among those who may need it. It also states that jails must facilitate continuation of medications after detainees are released.
Any number of factors may either facilitate or hinder the implementation of such a mandate, including leadership and staffing within the jail and collaborations with community-based organizations. In this study, the research team interviewed jail staff and held focus groups to learn about the facilitators and barriers to implementing the mandate in Massachusetts during the first year. Understanding what is needed to effectively implement medications for opioid use disorder in jails and link individuals to treatment upon release can help inform new policies and programming, thereby ultimately reducing risk for overdose and death.
HOW WAS THIS STUDY CONDUCTED?
The research team interviewed and held focus groups with jail staff about their perspectives regarding the first year of implementing the state legislative mandate in Massachusetts to provide access to medications for opioid use disorders in jails. The research was conducted across 7 Massachusetts county jails that had complied with the legislative mandate to expand access to medications approved by the Food and Drug Administration (FDA) to treat opioid use disorder. In particular, access to buprenorphine and methadone was expanded, given that these facilities were already providing access to naltrexone.
The research team conducted interviews and focus groups. Senior jail staff were interviewed individually, and other staff participated in the focus groups, which ranged in size from 2-11 participants. Interviews and focus groups were recorded so they could later be transcribed and coded for themes that emerged from participants’ responses. The research team coded the responses using standard qualitative methods and categories.
Outcomes of interest include internal and external contextual factors that influenced implementation of the mandate. External, or outer, factors included service environment, funding, and characteristics of the service recipients, while internal, or inner, factors included organizational characteristics and leadership, fidelity monitoring, and staff perspectives and hiring practices. Bridging factors were also examined, which included relationships between and within organizations, as well as relationships with community providers.
Participants included 61 clinical, corrections, and senior administrative staff who were recommended by jail administrators because of their involvement with decision-making regarding implementation of the policy. Most identified as White (80.3%) and as female (60.7%), with a mean age of 45 and a master’s degree level of education (45.9%). Many of the participants’ jobs involved behavioral health or addiction treatment (38.6%) or were administrative (29.8%). Among these, 27.3% had been working in their current position for less than 1 year, 25.5% had been for 1-3 years, and 32.7% had been for 4-9 years. Only 12.7% had been in their current position for more than 10 years. However, many of the participants had been working in their current agency for more than 10 years (41.8%) or 4-9 years (36.4%).
WHAT DID THIS STUDY FIND?
The broader political climate and funding helped facilitate implementation.
Implementation occurred during national and statewide shifts towards greater acceptance of treating opioid use disorder with medications. These shifts are evident by the mandate and by the state court’s ruling that failure to provide methadone violated constitutional rights, which occurred during the same time. Participants described how these broader shifts helped lead to acceptance among jail staff, particularly among newer and younger staff, and a “culture shift” from viewing medication treatment as illicit to necessary.
Participants also discussed how funding provided by the mandate was helpful for administering the medications and ensuring medication treatment would be continued after release.
Collaborations within and between organizations improved problem solving and efficiency.
Participants described how implementation helped to build collaborations between disciplines within the organization, which led to a more “cohesive” jail and the ability to develop solutions to problems. Likewise, collaborating with community-based organizations that they had established and trusting relationships with helped them solve problems and reduced the burden of developing new contracts and training new staff to implement the mandate.
Most participants said that collaboration with the state agency overseeing implementation was important to develop trust and identify practical limitations. However, some staff mentioned that they felt that the state agency did not sufficiently consider their perspectives.
Institutional policies, procedures, and training improve implementation.
Participants discussed the need for institutional policy and procedures to implement the mandate, with a key challenge being the determination of how to and who would administer medications. For instance, an important decision point was whether to develop an onsite treatment program or transport people offsite. This is because certain medications, such as methadone and buprenorphine, are subject to specific state and federal regulations (e.g., methadone be administered in a licensed facility; buprenorphine must be prescribed by a physician with specialized training).
Further, although many staff were accepting of the program, some staff, like medical staff, were concerned about “substituting one addiction for another.” However, participants discussed how this was alleviated with training and the fact that it was offered along with psychosocial therapy. Younger staff also tended to be more accepting of the program, which may be because they grew up during the opioid overdose epidemic and were most impacted. The growing shift towards a public health approach to addiction, as opposed to punitive approaches, that they grew up with also likely influenced their openness to agonist medications.
Finally, participants described how important it was for organizational leadership to listen to, and incorporate, feedback from staff. Leaders discussed how they worked to break down traditional power hierarchies and silos to encourage open communication about implementation and guide adaptations of existing procedures as needed.
Additional challenges with implementation were highlighted.
Participants discussed how confusion around sentencing and release dates made coordinating continuation of care challenging. Specifically,the main issues included not knowing whether pre-trial individuals would be sentenced, and if sentenced, not knowing people’s release dates,as well asnot knowing who might end up in a facility without access to medications. In addition, the burdensome and redundant nature of the reporting requirements was a challenge, but staff recognized the importance of it.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study interviewed jail staff to understand their perspectives regarding barriers and facilitators of the state legislative mandate in Massachusetts to provide access to medications for opioid use disorders in jails. Staff participants highlighted key facilitators of implementation involving the broader political climate, funding, and collaborations within and between organizations. A number of barriers and challenges were also highlighted, however, including the need for policies and procedures regarding how to and who will administer medications, the importance of staff training and education, and the importance of flexibility from leadership to adapt existing procedures according to staff feedback. Uncertainty around sentencing and release dates, as well as burdensome reporting requirements, were mentioned as additional challenges with implementation.
These findings are consistent with similar research conducted around the same time, but with correctional facilities across the US that were voluntarily providing access to medication for opioid use disorder. Notably, both sets of results, along with additional research, highlighted the challenges of adhering to state and federal regulations regarding agonist medication administration, the crucial importance of leadership and collaboration, and the growing culture shifts towards greater acceptance of medication treatment. An important difference, however, was that participants from facilities that offered medications voluntarily mentioned a lack of funding as a key barrier, while participants from facilities in Massachusetts that were mandated to offer medications discussed how funding was a key facilitator. This underscores the need for policies that allocate adequate funds for implementation.
Results from this study add to a growing number of studies providing consensus about what is needed to effectively implement medications for opioid use disorder in jails and link individuals to treatment upon release. Taken together, this research can help inform new policies and programming. For example, the strict regulations regarding administration of methadone may need to be relaxed or adapted for jail settings. Further, while the broader political environment helped to promote acceptance of medication treatment, staff training and education are needed to continue to reduce stigma and grow acceptance. Finally, since implementation requires collaboration with community-based organizations, preparing for implementation may involve a capacity-building phase where opportunities for collaboration are pursued.
Ultimately, understanding these barriers and facilitators can inform policies and programming, which can lead to effective and widespread implementation of providing access to medication for opioid use disorder in jails. This can help address the high-risk period for overdose following release and prevent deaths.
Participants were interviewed about their experiences with implementation during the first year of the mandate. As such, participants responses reflected factors that influenced preparation for and initiation of implementation. Responses from interviews conducted later will likely change to reflect how staff are working to sustain the program and their perspectives on potential outcomes.
Participants were staff who were recommended for recruitment because of their involvement with decision-making regardingimplementation of the policy. Therefore, they may have been biased towards its success and responded accordingly and could only offer insights from their specific viewpoint. Other staff who were not involved in decision-making may have had different perspectives and provided different responses.
There may have also been differences between staff roles and amount of time worked at the organization, but these potential differences were not examined due to the limitations in the study design.
The study took place in a northeast state in the US that had adequate resources and support. Results from the study therefore may not generalize to other states or countries with less resources and support.
BOTTOM LINE
Results from this study highlighted both barriers to and facilitators ofimplementingthe state legislative mandate in Massachusetts to provide access to medications for opioid use disorders in jails. Understanding these factors can inform policies and programming, which can ultimately help address the high-risk period for overdose following release and prevent deaths.
For individuals and families seeking recovery: Medication treatment during incarceration is not yet widely available in correctional settings.However, individuals who have the opportunity to take advantage of medication offerings where available are likely to have a lower risk for overdose upon release and potentially a higher likelihood of entering treatment. If not available during incarceration, however, individuals who begin medication treatment after their release are likely to experience similar benefits.
For treatment professionals and treatment systems: Jail systems that have the goal of implementing access to medications for opioid use disorder, or are in the beginning phases of implementation, can use the findings from this study to help guide them.Providing staff training and education, incorporating staff feedback into the adaptation of existing procedures, and collaborating within and between organizations are all likely to help implementation. If implementation is not feasible, however, jail administrators who provide individuals with opioid use disorder information about the risks of overdose upon release and how to obtain medication treatment may also help to prevent overdoses and deaths.
For scientists: While there have been a number of qualitative studies conducted to understand the barriers and facilitators to implementation of access to medication in jails, quantitative research and additional qualitative research in a variety of states with more limited resources will help us to understand the extent to which these results generalize. Perspectives from staff who were not involved in the decision-making process will also help to provide a more comprehensive understanding of the factors that influenced implementation. Finally, research that examines barriers and facilitators during a later stage of implementation will shed light on the factors that influence sustaining the program and potential outcomes.
For policy makers: Results from this study highlighted two important and actionable recommendations for policy makers. First, relaxing or adapting the strict regulations regarding administration of agonist medications in jail settings can help address this challenge to effective and streamlined implementation. Second, policies that allocate funding for implementation of access to medication in jails can help expand medication treatment programs in jails, thereby reducing risk of overdose and death following release.
Individuals with opioid use disorder who have been incarcerated are at an increased risk for overdose and death upon release. This is because abstinence during incarceration leads to decreased tolerance. Then, if individuals begin to use again upon release at the same level they did before incarceration, their risk for overdose is greatly increased.
Medications for opioid use disorder that are administered during incarceration can be helpful in preventing overdoses upon release, as well as leading to treatment entry and reducing risky behaviors, such as syringe sharing, which can increase risk of infectious disease transmission. However, while some jails and prisons are beginning to offer medications for opioid use disorder, it is still not a routine practice. This may be due to logistical barriers, such as the need for licensed medical staff and expenses. Of note, the administration of opioid agonist medications, such as methadone and buprenorphine, is subject to specific state and federal regulations that antagonist medications (e.g., naltrexone) are not. For instance, methadone must be administered in a licensed facility and, until recently, buprenorphine must be prescribed by a physician with specialized training. These regulations likely make medication administration in jail settings difficult.
In 2018, Massachusetts became the first state in the US to pass a legislative mandate to pilot the provision of access to medications for opioid use disorder in jails. This mandate states that medications must be maintained in individuals who were receiving it before being detained and initiated among those who may need it. It also states that jails must facilitate continuation of medications after detainees are released.
Any number of factors may either facilitate or hinder the implementation of such a mandate, including leadership and staffing within the jail and collaborations with community-based organizations. In this study, the research team interviewed jail staff and held focus groups to learn about the facilitators and barriers to implementing the mandate in Massachusetts during the first year. Understanding what is needed to effectively implement medications for opioid use disorder in jails and link individuals to treatment upon release can help inform new policies and programming, thereby ultimately reducing risk for overdose and death.
HOW WAS THIS STUDY CONDUCTED?
The research team interviewed and held focus groups with jail staff about their perspectives regarding the first year of implementing the state legislative mandate in Massachusetts to provide access to medications for opioid use disorders in jails. The research was conducted across 7 Massachusetts county jails that had complied with the legislative mandate to expand access to medications approved by the Food and Drug Administration (FDA) to treat opioid use disorder. In particular, access to buprenorphine and methadone was expanded, given that these facilities were already providing access to naltrexone.
The research team conducted interviews and focus groups. Senior jail staff were interviewed individually, and other staff participated in the focus groups, which ranged in size from 2-11 participants. Interviews and focus groups were recorded so they could later be transcribed and coded for themes that emerged from participants’ responses. The research team coded the responses using standard qualitative methods and categories.
Outcomes of interest include internal and external contextual factors that influenced implementation of the mandate. External, or outer, factors included service environment, funding, and characteristics of the service recipients, while internal, or inner, factors included organizational characteristics and leadership, fidelity monitoring, and staff perspectives and hiring practices. Bridging factors were also examined, which included relationships between and within organizations, as well as relationships with community providers.
Participants included 61 clinical, corrections, and senior administrative staff who were recommended by jail administrators because of their involvement with decision-making regarding implementation of the policy. Most identified as White (80.3%) and as female (60.7%), with a mean age of 45 and a master’s degree level of education (45.9%). Many of the participants’ jobs involved behavioral health or addiction treatment (38.6%) or were administrative (29.8%). Among these, 27.3% had been working in their current position for less than 1 year, 25.5% had been for 1-3 years, and 32.7% had been for 4-9 years. Only 12.7% had been in their current position for more than 10 years. However, many of the participants had been working in their current agency for more than 10 years (41.8%) or 4-9 years (36.4%).
WHAT DID THIS STUDY FIND?
The broader political climate and funding helped facilitate implementation.
Implementation occurred during national and statewide shifts towards greater acceptance of treating opioid use disorder with medications. These shifts are evident by the mandate and by the state court’s ruling that failure to provide methadone violated constitutional rights, which occurred during the same time. Participants described how these broader shifts helped lead to acceptance among jail staff, particularly among newer and younger staff, and a “culture shift” from viewing medication treatment as illicit to necessary.
Participants also discussed how funding provided by the mandate was helpful for administering the medications and ensuring medication treatment would be continued after release.
Collaborations within and between organizations improved problem solving and efficiency.
Participants described how implementation helped to build collaborations between disciplines within the organization, which led to a more “cohesive” jail and the ability to develop solutions to problems. Likewise, collaborating with community-based organizations that they had established and trusting relationships with helped them solve problems and reduced the burden of developing new contracts and training new staff to implement the mandate.
Most participants said that collaboration with the state agency overseeing implementation was important to develop trust and identify practical limitations. However, some staff mentioned that they felt that the state agency did not sufficiently consider their perspectives.
Institutional policies, procedures, and training improve implementation.
Participants discussed the need for institutional policy and procedures to implement the mandate, with a key challenge being the determination of how to and who would administer medications. For instance, an important decision point was whether to develop an onsite treatment program or transport people offsite. This is because certain medications, such as methadone and buprenorphine, are subject to specific state and federal regulations (e.g., methadone be administered in a licensed facility; buprenorphine must be prescribed by a physician with specialized training).
Further, although many staff were accepting of the program, some staff, like medical staff, were concerned about “substituting one addiction for another.” However, participants discussed how this was alleviated with training and the fact that it was offered along with psychosocial therapy. Younger staff also tended to be more accepting of the program, which may be because they grew up during the opioid overdose epidemic and were most impacted. The growing shift towards a public health approach to addiction, as opposed to punitive approaches, that they grew up with also likely influenced their openness to agonist medications.
Finally, participants described how important it was for organizational leadership to listen to, and incorporate, feedback from staff. Leaders discussed how they worked to break down traditional power hierarchies and silos to encourage open communication about implementation and guide adaptations of existing procedures as needed.
Additional challenges with implementation were highlighted.
Participants discussed how confusion around sentencing and release dates made coordinating continuation of care challenging. Specifically,the main issues included not knowing whether pre-trial individuals would be sentenced, and if sentenced, not knowing people’s release dates,as well asnot knowing who might end up in a facility without access to medications. In addition, the burdensome and redundant nature of the reporting requirements was a challenge, but staff recognized the importance of it.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Researchers in this study interviewed jail staff to understand their perspectives regarding barriers and facilitators of the state legislative mandate in Massachusetts to provide access to medications for opioid use disorders in jails. Staff participants highlighted key facilitators of implementation involving the broader political climate, funding, and collaborations within and between organizations. A number of barriers and challenges were also highlighted, however, including the need for policies and procedures regarding how to and who will administer medications, the importance of staff training and education, and the importance of flexibility from leadership to adapt existing procedures according to staff feedback. Uncertainty around sentencing and release dates, as well as burdensome reporting requirements, were mentioned as additional challenges with implementation.
These findings are consistent with similar research conducted around the same time, but with correctional facilities across the US that were voluntarily providing access to medication for opioid use disorder. Notably, both sets of results, along with additional research, highlighted the challenges of adhering to state and federal regulations regarding agonist medication administration, the crucial importance of leadership and collaboration, and the growing culture shifts towards greater acceptance of medication treatment. An important difference, however, was that participants from facilities that offered medications voluntarily mentioned a lack of funding as a key barrier, while participants from facilities in Massachusetts that were mandated to offer medications discussed how funding was a key facilitator. This underscores the need for policies that allocate adequate funds for implementation.
Results from this study add to a growing number of studies providing consensus about what is needed to effectively implement medications for opioid use disorder in jails and link individuals to treatment upon release. Taken together, this research can help inform new policies and programming. For example, the strict regulations regarding administration of methadone may need to be relaxed or adapted for jail settings. Further, while the broader political environment helped to promote acceptance of medication treatment, staff training and education are needed to continue to reduce stigma and grow acceptance. Finally, since implementation requires collaboration with community-based organizations, preparing for implementation may involve a capacity-building phase where opportunities for collaboration are pursued.
Ultimately, understanding these barriers and facilitators can inform policies and programming, which can lead to effective and widespread implementation of providing access to medication for opioid use disorder in jails. This can help address the high-risk period for overdose following release and prevent deaths.
Participants were interviewed about their experiences with implementation during the first year of the mandate. As such, participants responses reflected factors that influenced preparation for and initiation of implementation. Responses from interviews conducted later will likely change to reflect how staff are working to sustain the program and their perspectives on potential outcomes.
Participants were staff who were recommended for recruitment because of their involvement with decision-making regardingimplementation of the policy. Therefore, they may have been biased towards its success and responded accordingly and could only offer insights from their specific viewpoint. Other staff who were not involved in decision-making may have had different perspectives and provided different responses.
There may have also been differences between staff roles and amount of time worked at the organization, but these potential differences were not examined due to the limitations in the study design.
The study took place in a northeast state in the US that had adequate resources and support. Results from the study therefore may not generalize to other states or countries with less resources and support.
BOTTOM LINE
Results from this study highlighted both barriers to and facilitators ofimplementingthe state legislative mandate in Massachusetts to provide access to medications for opioid use disorders in jails. Understanding these factors can inform policies and programming, which can ultimately help address the high-risk period for overdose following release and prevent deaths.
For individuals and families seeking recovery: Medication treatment during incarceration is not yet widely available in correctional settings.However, individuals who have the opportunity to take advantage of medication offerings where available are likely to have a lower risk for overdose upon release and potentially a higher likelihood of entering treatment. If not available during incarceration, however, individuals who begin medication treatment after their release are likely to experience similar benefits.
For treatment professionals and treatment systems: Jail systems that have the goal of implementing access to medications for opioid use disorder, or are in the beginning phases of implementation, can use the findings from this study to help guide them.Providing staff training and education, incorporating staff feedback into the adaptation of existing procedures, and collaborating within and between organizations are all likely to help implementation. If implementation is not feasible, however, jail administrators who provide individuals with opioid use disorder information about the risks of overdose upon release and how to obtain medication treatment may also help to prevent overdoses and deaths.
For scientists: While there have been a number of qualitative studies conducted to understand the barriers and facilitators to implementation of access to medication in jails, quantitative research and additional qualitative research in a variety of states with more limited resources will help us to understand the extent to which these results generalize. Perspectives from staff who were not involved in the decision-making process will also help to provide a more comprehensive understanding of the factors that influenced implementation. Finally, research that examines barriers and facilitators during a later stage of implementation will shed light on the factors that influence sustaining the program and potential outcomes.
For policy makers: Results from this study highlighted two important and actionable recommendations for policy makers. First, relaxing or adapting the strict regulations regarding administration of agonist medications in jail settings can help address this challenge to effective and streamlined implementation. Second, policies that allocate funding for implementation of access to medication in jails can help expand medication treatment programs in jails, thereby reducing risk of overdose and death following release.