Stigma and addiction: Providing genetic explanations for alcohol use or gambling disorder does not improve addiction provider attitudes and treatment expectations
Stigma and addiction: Providing genetic explanations for alcohol use or gambling disorder does not improve addiction provider attitudes and treatment expectations
Biomedical terminology has been purposely used to describe addiction in hopes it would reduce stigma, though it could also have the unintended consequence of limiting expectations that treatment can help. In this study, researchers tested whether genetic explanations of alcohol use disorder and gambling disorder impact addiction treatment providers’ attitudes and expectations of recovery.
Perceived stigma may be a barrier to seeking care for individuals with both alcohol use disorder and/or gambling disorder, which may be delaying and preventing treatment. In fact, words used to describe substance use disorders have been shown to affect the level of perceived stigma by healthcare professionals and the general public. For example, among the general public and mental health clinicians, the term ‘substance abuser’ tends to elicit a more punitive attitude toward an individual with substance use-related problems whereas the term ‘substance use disorder’ tends to elicit a more treatment-oriented attitude. Efforts to emphasize the biophysiological elements of substance use disorders have proliferated, in part, because they are thought to reduce stigmatizing attitudes toward these individuals. Indeed, for individuals with opioid use disorder, for example, referring to such individuals as having a “chronically relapsing brain disease” reduces stigmatizing blame. At the same time, referring to such individuals as having an opioid “problem”, compared to disease terminology, increases expectations that individuals will recover (i.e., this term produces higher perceived “prognostic optimism”) and reduces levels of perceived danger. Similar efforts to understand how genetic attributions for substance use and related conditions impact perceptions of such individuals can inform public health messaging.
Much of the research on factors impacting stigmatizing attitudes has been conducted on alcohol, opioid, and other substance use disorders. Gambling disorders have taken on added public health significance after sports gambling has been legalized and scaled with readily accessible online platforms. If the implications of using genetic attributions to explain alcohol use disorder and gambling disorder were better understood, we could better tailor guidelines to improve participant engagement and outcomes.
HOW WAS THIS STUDY CONDUCTED?
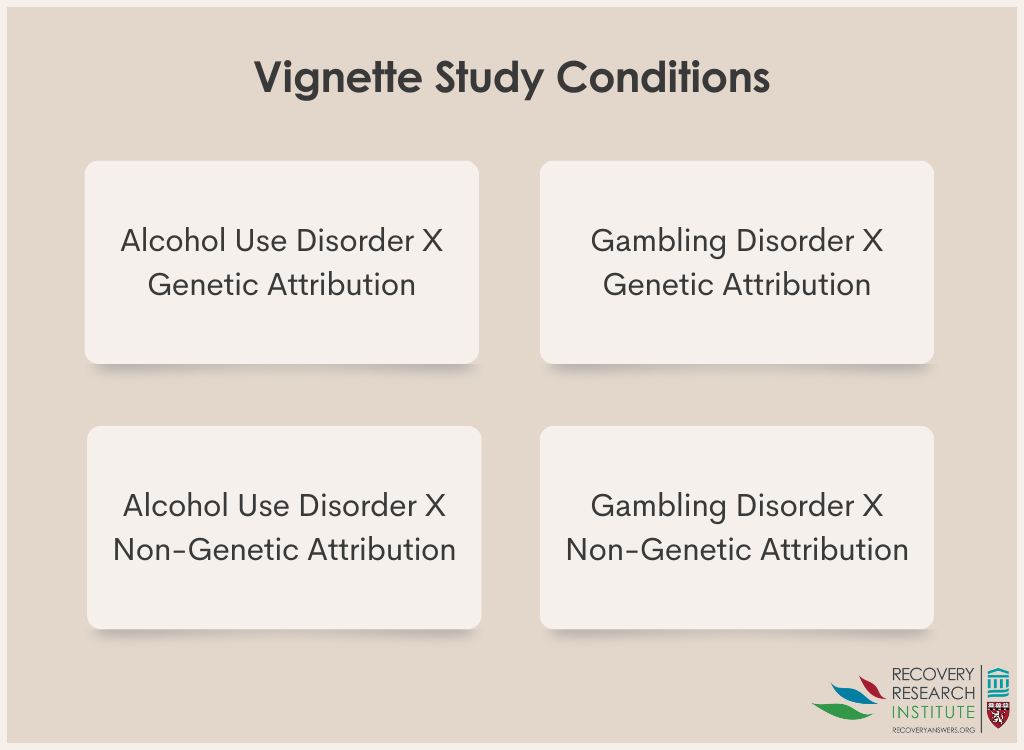
This was a study of addiction treatment providers from 4 professional organizations – one for addiction medicine physicians, one for addiction psychiatrists, one for addiction psychologists, and one for addiction counselors. The goal was to investigate the impact of providing genetic explanations for disorders on the attitudes and beliefs of treatment providers. The researchers provided addiction professionals with a description of a fictious patient with alcohol use disorder or gambling disorder, experimentally varied whether this was attributed to genetic causes (see Figure below), and then gauged their reactions to the patient.
Description of Vignette
Providers were randomly assigned to read that a patient named “Charlie” had been diagnosed with either an alcohol use disorder or gambling disorder. They read that Charlie recently underwent state-of-the-art genetic testing, and were told either that “Charlie has a genetic predisposition” to his disorder, suggesting that his symptoms “likely stem from his DNA” or that he has no such genetic predisposition, suggesting no genetic cause for his symptoms.
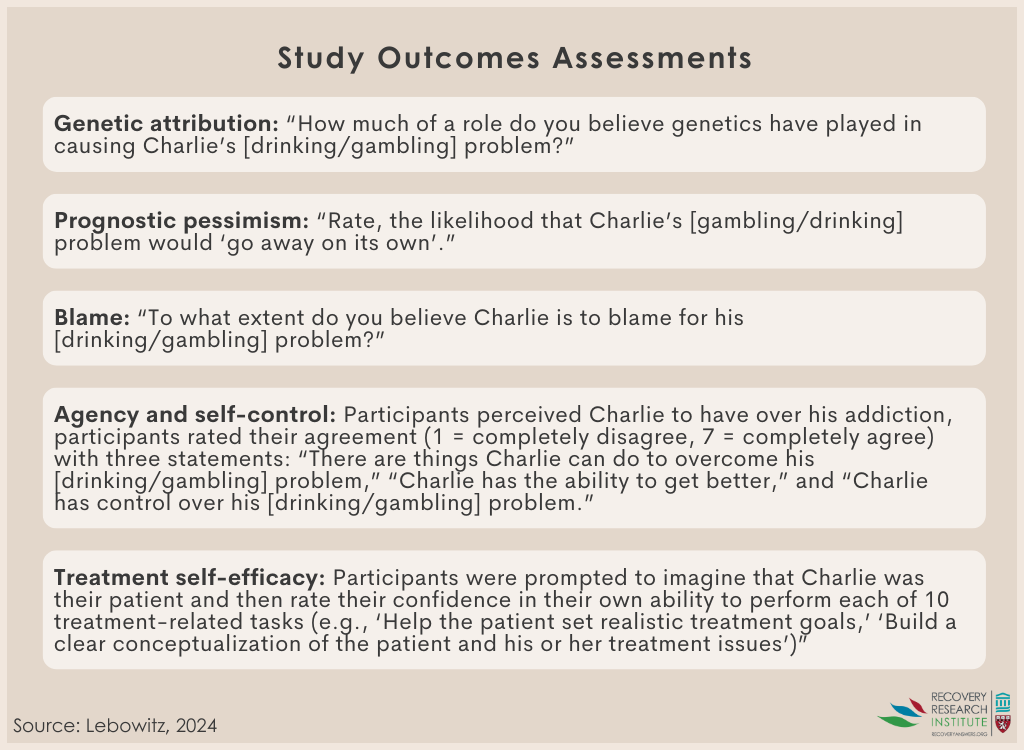
The study variables can be organized into four main sections: experimental manipulations (i.e., independent variables), outcomes, moderators, and a manipulation check. The experimental manipulations included two variables (see Figure above): genetic information (genetic predisposition versus no genetic predisposition described) and disorder (alcohol use disorder versus gambling disorder). The outcomes included nine variables (see Figure below for examples): 1) blame (example question: To what extent do you believe the patient is to blame for his [drinking/gambling] problem?), 2) effectiveness of medication (example question: Rate the likelihood that the patient’s [drinking/gambling] problem would “get better” if treated with medication), 3) effectiveness of psychotherapy (example question: rate the likelihood that the patient’s [drinking/gambling] problem would “get better” if treated with psychotherapy), 4) prognostic pessimism (example question: how permanent do you believe the patient’s [gambling/drinking] problem to be? also examined as- example question: likelihood the patient’s substance use disorder will “go away”), 5) patient agency (example question: there are things the patient can do to overcome his [drinking/gambling] problem), 6) patient self-control (example question: control over [gambling/drinking] problem), 7) empathy (example question: how much does compassion describe your feelings about the patient), 8) social distance (example question: how much would you like to work closely together on a job), and 9) treatment self-efficacy (example question: rate your ability to set realistic treatment goals).
The researchers hypothesized that that genetic explanations would be associated with reduced blame and increased confidence in the effectiveness of medication, but also with greater prognostic pessimism and diminished perceptions of the patient’s self-control and agency and the effectiveness of psychotherapy. They also examined the relationship between genetic explanations and empathy, social distance, and confidence in the providers’ ability to effectively treat the patient.
The professional training background of the sample included addiction professionals with both medical (n = 153) and nonmedical (n = 232) backgrounds. Participants reported a mean of 17 years of experience treating patients with addictive disorders and an average of 17 hours per week spent treating patients with addictive disorders.
WHAT DID THIS STUDY FIND?
Genetic explanations did not alter provider attitudes or expectations, though other factors made a difference
Contrary to the hypotheses, genetic explanations of a patient’s symptoms for alcohol use disorder or gambling disorder did not impact any of the outcomes. The presence of an alcohol use disorder versus a gambling disorder did affect provider beliefs about the efficacy of psychotherapy or medication. Specifically, providers rated the patient as more likely to benefit from psychotherapy when he was described as having gambling disorder compared to alcohol use disorder. Alternatively, providers rated the patient as more likely to benefit from medication when he was described as having an alcohol use disorder compared to a gambling disorder.
Irrespective of condition, providers with medical degrees were more likely to attribute genetic causes
Compared to participants with a nonmedical background, those with a medical background had significantly stronger genetic attributions for the patient’s disorder, were less confident the patient would benefit from psychotherapy, perceived the patient’s disorder as more permanent, perceived the patient to have less agency and self-control, attributed less blame to the patient, and had lower empathy and treatment self-efficacy.
Stronger genetic attributions were correlated with attitudes and beliefs in expected ways
After controlling for participants’ assigned condition (genetic versus nongenetic explanation) and disorder presented in the vignette (alcohol use disorder versus gambling disorder), the researchers examined if clinicians’ genetic attributions independent of the experimental manipulation (i.e., “genetic explanation” vs. “no genetic explanation”) were correlated to their responses on other measures. They found that participants’ genetic attributions for the patient’s symptoms were associated with reduced blame on the patient and increased belief in the effectiveness of medication, but also with reduced confidence in the effectiveness of psychotherapy and with pessimism about the patient’s prognosis.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that confirming the presence or absence of a genetic explanation for patient symptoms of alcohol use disorder or gambling disorder did not affect addiction providers’ attitudes toward patients or clinically relevant beliefs and perceptions. It is not entirely clear why the vignette describing a genetic explanation for the patient’s alcohol or gambling disorder did not impact stigmatizing attitudes as has been shown in other studies. It may be that, for this group of trained addiction providers, their attitudes and beliefs were well formed based on knowledge and experience; shifting them with differing etiological explanations may be more challenging than among the general public, for example. Despite not showing any effect of the genetic explanation on provider attitudes, the study offered other insights.
Compared to participants with a nonmedical background, providers with a medical background had significantly stronger genetic attributions for the patient’s disorder, were less confident the patient would benefit from psychotherapy, perceived the patient’s disorder as more permanent, perceived the patient to have less agency and self-control, attributed less blame to the patient, and had lower empathy and treatment self-efficacy. To the extent that providers with a medical background attribute substance use disorder and gambling disorder to genetics, they may be likely to prescribe medication without considering the utility of various psychotherapies. While less patient blame is needed to reduce stigma, the perception of a patient having less agency, self-control, or being afflicted with a condition that their provider considers to be permanent may undermine expectations for recovery and hamper the patient’s willingness to seek care or envision a more hopeful future.
Alternatively, the presence of an alcohol use disorder versus a gambling disorder did affect provider beliefs about the efficacy of psychotherapy or medication. Clinicians rated the patient as more likely to benefit from psychotherapy when he was described as having gambling disorder compared to alcohol use disorder. Additionally, providers rated the patient as more likely to benefit from medication when he was described as having an alcohol use disorder compared to a gambling disorder. These beliefs may be shaped by the current landscape of treatment options given there is no FDA approved medications for gambling disorder and yet several options for alcohol use disorder exist, while psychotherapy can be used to treat either alcohol use disorder or gambling disorder. Also, because alcohol is a psychoactive substance that causes direct neurotoxic effects as well as profound neurobiological adaptations, professionals may view its effects as more “biological” than gambling disorder and thus be more likely to be in favor of a medication to treat it.
Though participants spent 17 hours per week treating patients with “addictive disorders”, the extent to which they have ever treated patients with a gambling disorder was unclear.
Like most studies in the area of language and stigma, this was a vignette-based study of attitudes and beliefs. It is unclear the extent to which such beliefs and attitudes affect real world behaviors or policies.
This study found that confirming the presence or absence of a genetic explanation for patient symptoms of alcohol use disorder or gambling disorder did not affect addiction providers’ or clinicians’ attitudes toward patients or clinically relevant beliefs and perceptions, though other findings were informative. For example, compared to participants with a nonmedical background, those with a medical background had significantly stronger genetic attributions for the patient’s disorder, were less confident the patient would benefit from psychotherapy, perceived the patient’s disorder as more permanent, perceived the patient to have less agency and self-control, attributed less blame to the patient, and had lower empathy and treatment self-efficacy. This study adds to the large and growing body of research on the impacts that terminology and causal explanations for substance use are important to understanding stigmatizing attitudes and recovery expectations.
For individuals and families seeking recovery: Disorders are affected by many factors including genetic attribution. This study focused on how providers’ perceptions of their patients were affected by confirming the presence of a genetic attribution. Whether a provider has a medical or non-medical background may influence their treatment approach and perception about likelihood of recovery from substance use and gambling disorders. Keep in mind that which treatment approach (medical vs non-medical) may be best is beyond the scope of this study.
For treatment professionals and treatment systems: This study found that providers with medical versus nonmedical backgrounds may respond differently to genetic attributions of disorder that can affect their beliefs about the treatment of alcohol use and gambling disorders. It is important that providers consider how their perceptions are communicated to patients and how that may impact patient behavior.
For scientists: This study focused on the impact of providing genetic explanations of alcohol and gambling disorder and how that shapes perception of providers with both medical and non-medical backgrounds. The extent to which these results generalize to interactions between family members and people with a disorder or public health messaging is unknown and should be investigated.
For policy makers: Genetic testing for substance use disorders is a tool to being used in precision medicine, which aims to understand how genes influence health and allow for customized intervention. This study examined the impact of having a genetic explanation for alcohol and gambling disorder impacted providers’ perceptions of their patients. Findings showed a genetic explanation did not affect addiction providers’ or clinicians’ attitudes toward patients or clinically relevant beliefs and perceptions. It may be that, for this group of trained addiction providers, their attitudes and beliefs were well formed based on knowledge and experience; shifting them with differing etiological explanations may be more challenging than among the general public, for example. Funding for studies that examine ideal terms and conceptual frameworks to reduce stigma toward individuals with substance use and related disorders is likely to improve individuals’ engagement with treatment and recovery supports and ultimately reduce the disease burden of alcohol and other drug use disorders.
Perceived stigma may be a barrier to seeking care for individuals with both alcohol use disorder and/or gambling disorder, which may be delaying and preventing treatment. In fact, words used to describe substance use disorders have been shown to affect the level of perceived stigma by healthcare professionals and the general public. For example, among the general public and mental health clinicians, the term ‘substance abuser’ tends to elicit a more punitive attitude toward an individual with substance use-related problems whereas the term ‘substance use disorder’ tends to elicit a more treatment-oriented attitude. Efforts to emphasize the biophysiological elements of substance use disorders have proliferated, in part, because they are thought to reduce stigmatizing attitudes toward these individuals. Indeed, for individuals with opioid use disorder, for example, referring to such individuals as having a “chronically relapsing brain disease” reduces stigmatizing blame. At the same time, referring to such individuals as having an opioid “problem”, compared to disease terminology, increases expectations that individuals will recover (i.e., this term produces higher perceived “prognostic optimism”) and reduces levels of perceived danger. Similar efforts to understand how genetic attributions for substance use and related conditions impact perceptions of such individuals can inform public health messaging.
Much of the research on factors impacting stigmatizing attitudes has been conducted on alcohol, opioid, and other substance use disorders. Gambling disorders have taken on added public health significance after sports gambling has been legalized and scaled with readily accessible online platforms. If the implications of using genetic attributions to explain alcohol use disorder and gambling disorder were better understood, we could better tailor guidelines to improve participant engagement and outcomes.
HOW WAS THIS STUDY CONDUCTED?
This was a study of addiction treatment providers from 4 professional organizations – one for addiction medicine physicians, one for addiction psychiatrists, one for addiction psychologists, and one for addiction counselors. The goal was to investigate the impact of providing genetic explanations for disorders on the attitudes and beliefs of treatment providers. The researchers provided addiction professionals with a description of a fictious patient with alcohol use disorder or gambling disorder, experimentally varied whether this was attributed to genetic causes (see Figure below), and then gauged their reactions to the patient.
Description of Vignette
Providers were randomly assigned to read that a patient named “Charlie” had been diagnosed with either an alcohol use disorder or gambling disorder. They read that Charlie recently underwent state-of-the-art genetic testing, and were told either that “Charlie has a genetic predisposition” to his disorder, suggesting that his symptoms “likely stem from his DNA” or that he has no such genetic predisposition, suggesting no genetic cause for his symptoms.
The study variables can be organized into four main sections: experimental manipulations (i.e., independent variables), outcomes, moderators, and a manipulation check. The experimental manipulations included two variables (see Figure above): genetic information (genetic predisposition versus no genetic predisposition described) and disorder (alcohol use disorder versus gambling disorder). The outcomes included nine variables (see Figure below for examples): 1) blame (example question: To what extent do you believe the patient is to blame for his [drinking/gambling] problem?), 2) effectiveness of medication (example question: Rate the likelihood that the patient’s [drinking/gambling] problem would “get better” if treated with medication), 3) effectiveness of psychotherapy (example question: rate the likelihood that the patient’s [drinking/gambling] problem would “get better” if treated with psychotherapy), 4) prognostic pessimism (example question: how permanent do you believe the patient’s [gambling/drinking] problem to be? also examined as- example question: likelihood the patient’s substance use disorder will “go away”), 5) patient agency (example question: there are things the patient can do to overcome his [drinking/gambling] problem), 6) patient self-control (example question: control over [gambling/drinking] problem), 7) empathy (example question: how much does compassion describe your feelings about the patient), 8) social distance (example question: how much would you like to work closely together on a job), and 9) treatment self-efficacy (example question: rate your ability to set realistic treatment goals).
The researchers hypothesized that that genetic explanations would be associated with reduced blame and increased confidence in the effectiveness of medication, but also with greater prognostic pessimism and diminished perceptions of the patient’s self-control and agency and the effectiveness of psychotherapy. They also examined the relationship between genetic explanations and empathy, social distance, and confidence in the providers’ ability to effectively treat the patient.
The professional training background of the sample included addiction professionals with both medical (n = 153) and nonmedical (n = 232) backgrounds. Participants reported a mean of 17 years of experience treating patients with addictive disorders and an average of 17 hours per week spent treating patients with addictive disorders.
WHAT DID THIS STUDY FIND?
Genetic explanations did not alter provider attitudes or expectations, though other factors made a difference
Contrary to the hypotheses, genetic explanations of a patient’s symptoms for alcohol use disorder or gambling disorder did not impact any of the outcomes. The presence of an alcohol use disorder versus a gambling disorder did affect provider beliefs about the efficacy of psychotherapy or medication. Specifically, providers rated the patient as more likely to benefit from psychotherapy when he was described as having gambling disorder compared to alcohol use disorder. Alternatively, providers rated the patient as more likely to benefit from medication when he was described as having an alcohol use disorder compared to a gambling disorder.
Irrespective of condition, providers with medical degrees were more likely to attribute genetic causes
Compared to participants with a nonmedical background, those with a medical background had significantly stronger genetic attributions for the patient’s disorder, were less confident the patient would benefit from psychotherapy, perceived the patient’s disorder as more permanent, perceived the patient to have less agency and self-control, attributed less blame to the patient, and had lower empathy and treatment self-efficacy.
Stronger genetic attributions were correlated with attitudes and beliefs in expected ways
After controlling for participants’ assigned condition (genetic versus nongenetic explanation) and disorder presented in the vignette (alcohol use disorder versus gambling disorder), the researchers examined if clinicians’ genetic attributions independent of the experimental manipulation (i.e., “genetic explanation” vs. “no genetic explanation”) were correlated to their responses on other measures. They found that participants’ genetic attributions for the patient’s symptoms were associated with reduced blame on the patient and increased belief in the effectiveness of medication, but also with reduced confidence in the effectiveness of psychotherapy and with pessimism about the patient’s prognosis.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that confirming the presence or absence of a genetic explanation for patient symptoms of alcohol use disorder or gambling disorder did not affect addiction providers’ attitudes toward patients or clinically relevant beliefs and perceptions. It is not entirely clear why the vignette describing a genetic explanation for the patient’s alcohol or gambling disorder did not impact stigmatizing attitudes as has been shown in other studies. It may be that, for this group of trained addiction providers, their attitudes and beliefs were well formed based on knowledge and experience; shifting them with differing etiological explanations may be more challenging than among the general public, for example. Despite not showing any effect of the genetic explanation on provider attitudes, the study offered other insights.
Compared to participants with a nonmedical background, providers with a medical background had significantly stronger genetic attributions for the patient’s disorder, were less confident the patient would benefit from psychotherapy, perceived the patient’s disorder as more permanent, perceived the patient to have less agency and self-control, attributed less blame to the patient, and had lower empathy and treatment self-efficacy. To the extent that providers with a medical background attribute substance use disorder and gambling disorder to genetics, they may be likely to prescribe medication without considering the utility of various psychotherapies. While less patient blame is needed to reduce stigma, the perception of a patient having less agency, self-control, or being afflicted with a condition that their provider considers to be permanent may undermine expectations for recovery and hamper the patient’s willingness to seek care or envision a more hopeful future.
Alternatively, the presence of an alcohol use disorder versus a gambling disorder did affect provider beliefs about the efficacy of psychotherapy or medication. Clinicians rated the patient as more likely to benefit from psychotherapy when he was described as having gambling disorder compared to alcohol use disorder. Additionally, providers rated the patient as more likely to benefit from medication when he was described as having an alcohol use disorder compared to a gambling disorder. These beliefs may be shaped by the current landscape of treatment options given there is no FDA approved medications for gambling disorder and yet several options for alcohol use disorder exist, while psychotherapy can be used to treat either alcohol use disorder or gambling disorder. Also, because alcohol is a psychoactive substance that causes direct neurotoxic effects as well as profound neurobiological adaptations, professionals may view its effects as more “biological” than gambling disorder and thus be more likely to be in favor of a medication to treat it.
Though participants spent 17 hours per week treating patients with “addictive disorders”, the extent to which they have ever treated patients with a gambling disorder was unclear.
Like most studies in the area of language and stigma, this was a vignette-based study of attitudes and beliefs. It is unclear the extent to which such beliefs and attitudes affect real world behaviors or policies.
This study found that confirming the presence or absence of a genetic explanation for patient symptoms of alcohol use disorder or gambling disorder did not affect addiction providers’ or clinicians’ attitudes toward patients or clinically relevant beliefs and perceptions, though other findings were informative. For example, compared to participants with a nonmedical background, those with a medical background had significantly stronger genetic attributions for the patient’s disorder, were less confident the patient would benefit from psychotherapy, perceived the patient’s disorder as more permanent, perceived the patient to have less agency and self-control, attributed less blame to the patient, and had lower empathy and treatment self-efficacy. This study adds to the large and growing body of research on the impacts that terminology and causal explanations for substance use are important to understanding stigmatizing attitudes and recovery expectations.
For individuals and families seeking recovery: Disorders are affected by many factors including genetic attribution. This study focused on how providers’ perceptions of their patients were affected by confirming the presence of a genetic attribution. Whether a provider has a medical or non-medical background may influence their treatment approach and perception about likelihood of recovery from substance use and gambling disorders. Keep in mind that which treatment approach (medical vs non-medical) may be best is beyond the scope of this study.
For treatment professionals and treatment systems: This study found that providers with medical versus nonmedical backgrounds may respond differently to genetic attributions of disorder that can affect their beliefs about the treatment of alcohol use and gambling disorders. It is important that providers consider how their perceptions are communicated to patients and how that may impact patient behavior.
For scientists: This study focused on the impact of providing genetic explanations of alcohol and gambling disorder and how that shapes perception of providers with both medical and non-medical backgrounds. The extent to which these results generalize to interactions between family members and people with a disorder or public health messaging is unknown and should be investigated.
For policy makers: Genetic testing for substance use disorders is a tool to being used in precision medicine, which aims to understand how genes influence health and allow for customized intervention. This study examined the impact of having a genetic explanation for alcohol and gambling disorder impacted providers’ perceptions of their patients. Findings showed a genetic explanation did not affect addiction providers’ or clinicians’ attitudes toward patients or clinically relevant beliefs and perceptions. It may be that, for this group of trained addiction providers, their attitudes and beliefs were well formed based on knowledge and experience; shifting them with differing etiological explanations may be more challenging than among the general public, for example. Funding for studies that examine ideal terms and conceptual frameworks to reduce stigma toward individuals with substance use and related disorders is likely to improve individuals’ engagement with treatment and recovery supports and ultimately reduce the disease burden of alcohol and other drug use disorders.
Perceived stigma may be a barrier to seeking care for individuals with both alcohol use disorder and/or gambling disorder, which may be delaying and preventing treatment. In fact, words used to describe substance use disorders have been shown to affect the level of perceived stigma by healthcare professionals and the general public. For example, among the general public and mental health clinicians, the term ‘substance abuser’ tends to elicit a more punitive attitude toward an individual with substance use-related problems whereas the term ‘substance use disorder’ tends to elicit a more treatment-oriented attitude. Efforts to emphasize the biophysiological elements of substance use disorders have proliferated, in part, because they are thought to reduce stigmatizing attitudes toward these individuals. Indeed, for individuals with opioid use disorder, for example, referring to such individuals as having a “chronically relapsing brain disease” reduces stigmatizing blame. At the same time, referring to such individuals as having an opioid “problem”, compared to disease terminology, increases expectations that individuals will recover (i.e., this term produces higher perceived “prognostic optimism”) and reduces levels of perceived danger. Similar efforts to understand how genetic attributions for substance use and related conditions impact perceptions of such individuals can inform public health messaging.
Much of the research on factors impacting stigmatizing attitudes has been conducted on alcohol, opioid, and other substance use disorders. Gambling disorders have taken on added public health significance after sports gambling has been legalized and scaled with readily accessible online platforms. If the implications of using genetic attributions to explain alcohol use disorder and gambling disorder were better understood, we could better tailor guidelines to improve participant engagement and outcomes.
HOW WAS THIS STUDY CONDUCTED?
This was a study of addiction treatment providers from 4 professional organizations – one for addiction medicine physicians, one for addiction psychiatrists, one for addiction psychologists, and one for addiction counselors. The goal was to investigate the impact of providing genetic explanations for disorders on the attitudes and beliefs of treatment providers. The researchers provided addiction professionals with a description of a fictious patient with alcohol use disorder or gambling disorder, experimentally varied whether this was attributed to genetic causes (see Figure below), and then gauged their reactions to the patient.
Description of Vignette
Providers were randomly assigned to read that a patient named “Charlie” had been diagnosed with either an alcohol use disorder or gambling disorder. They read that Charlie recently underwent state-of-the-art genetic testing, and were told either that “Charlie has a genetic predisposition” to his disorder, suggesting that his symptoms “likely stem from his DNA” or that he has no such genetic predisposition, suggesting no genetic cause for his symptoms.
The study variables can be organized into four main sections: experimental manipulations (i.e., independent variables), outcomes, moderators, and a manipulation check. The experimental manipulations included two variables (see Figure above): genetic information (genetic predisposition versus no genetic predisposition described) and disorder (alcohol use disorder versus gambling disorder). The outcomes included nine variables (see Figure below for examples): 1) blame (example question: To what extent do you believe the patient is to blame for his [drinking/gambling] problem?), 2) effectiveness of medication (example question: Rate the likelihood that the patient’s [drinking/gambling] problem would “get better” if treated with medication), 3) effectiveness of psychotherapy (example question: rate the likelihood that the patient’s [drinking/gambling] problem would “get better” if treated with psychotherapy), 4) prognostic pessimism (example question: how permanent do you believe the patient’s [gambling/drinking] problem to be? also examined as- example question: likelihood the patient’s substance use disorder will “go away”), 5) patient agency (example question: there are things the patient can do to overcome his [drinking/gambling] problem), 6) patient self-control (example question: control over [gambling/drinking] problem), 7) empathy (example question: how much does compassion describe your feelings about the patient), 8) social distance (example question: how much would you like to work closely together on a job), and 9) treatment self-efficacy (example question: rate your ability to set realistic treatment goals).
The researchers hypothesized that that genetic explanations would be associated with reduced blame and increased confidence in the effectiveness of medication, but also with greater prognostic pessimism and diminished perceptions of the patient’s self-control and agency and the effectiveness of psychotherapy. They also examined the relationship between genetic explanations and empathy, social distance, and confidence in the providers’ ability to effectively treat the patient.
The professional training background of the sample included addiction professionals with both medical (n = 153) and nonmedical (n = 232) backgrounds. Participants reported a mean of 17 years of experience treating patients with addictive disorders and an average of 17 hours per week spent treating patients with addictive disorders.
WHAT DID THIS STUDY FIND?
Genetic explanations did not alter provider attitudes or expectations, though other factors made a difference
Contrary to the hypotheses, genetic explanations of a patient’s symptoms for alcohol use disorder or gambling disorder did not impact any of the outcomes. The presence of an alcohol use disorder versus a gambling disorder did affect provider beliefs about the efficacy of psychotherapy or medication. Specifically, providers rated the patient as more likely to benefit from psychotherapy when he was described as having gambling disorder compared to alcohol use disorder. Alternatively, providers rated the patient as more likely to benefit from medication when he was described as having an alcohol use disorder compared to a gambling disorder.
Irrespective of condition, providers with medical degrees were more likely to attribute genetic causes
Compared to participants with a nonmedical background, those with a medical background had significantly stronger genetic attributions for the patient’s disorder, were less confident the patient would benefit from psychotherapy, perceived the patient’s disorder as more permanent, perceived the patient to have less agency and self-control, attributed less blame to the patient, and had lower empathy and treatment self-efficacy.
Stronger genetic attributions were correlated with attitudes and beliefs in expected ways
After controlling for participants’ assigned condition (genetic versus nongenetic explanation) and disorder presented in the vignette (alcohol use disorder versus gambling disorder), the researchers examined if clinicians’ genetic attributions independent of the experimental manipulation (i.e., “genetic explanation” vs. “no genetic explanation”) were correlated to their responses on other measures. They found that participants’ genetic attributions for the patient’s symptoms were associated with reduced blame on the patient and increased belief in the effectiveness of medication, but also with reduced confidence in the effectiveness of psychotherapy and with pessimism about the patient’s prognosis.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study found that confirming the presence or absence of a genetic explanation for patient symptoms of alcohol use disorder or gambling disorder did not affect addiction providers’ attitudes toward patients or clinically relevant beliefs and perceptions. It is not entirely clear why the vignette describing a genetic explanation for the patient’s alcohol or gambling disorder did not impact stigmatizing attitudes as has been shown in other studies. It may be that, for this group of trained addiction providers, their attitudes and beliefs were well formed based on knowledge and experience; shifting them with differing etiological explanations may be more challenging than among the general public, for example. Despite not showing any effect of the genetic explanation on provider attitudes, the study offered other insights.
Compared to participants with a nonmedical background, providers with a medical background had significantly stronger genetic attributions for the patient’s disorder, were less confident the patient would benefit from psychotherapy, perceived the patient’s disorder as more permanent, perceived the patient to have less agency and self-control, attributed less blame to the patient, and had lower empathy and treatment self-efficacy. To the extent that providers with a medical background attribute substance use disorder and gambling disorder to genetics, they may be likely to prescribe medication without considering the utility of various psychotherapies. While less patient blame is needed to reduce stigma, the perception of a patient having less agency, self-control, or being afflicted with a condition that their provider considers to be permanent may undermine expectations for recovery and hamper the patient’s willingness to seek care or envision a more hopeful future.
Alternatively, the presence of an alcohol use disorder versus a gambling disorder did affect provider beliefs about the efficacy of psychotherapy or medication. Clinicians rated the patient as more likely to benefit from psychotherapy when he was described as having gambling disorder compared to alcohol use disorder. Additionally, providers rated the patient as more likely to benefit from medication when he was described as having an alcohol use disorder compared to a gambling disorder. These beliefs may be shaped by the current landscape of treatment options given there is no FDA approved medications for gambling disorder and yet several options for alcohol use disorder exist, while psychotherapy can be used to treat either alcohol use disorder or gambling disorder. Also, because alcohol is a psychoactive substance that causes direct neurotoxic effects as well as profound neurobiological adaptations, professionals may view its effects as more “biological” than gambling disorder and thus be more likely to be in favor of a medication to treat it.
Though participants spent 17 hours per week treating patients with “addictive disorders”, the extent to which they have ever treated patients with a gambling disorder was unclear.
Like most studies in the area of language and stigma, this was a vignette-based study of attitudes and beliefs. It is unclear the extent to which such beliefs and attitudes affect real world behaviors or policies.
This study found that confirming the presence or absence of a genetic explanation for patient symptoms of alcohol use disorder or gambling disorder did not affect addiction providers’ or clinicians’ attitudes toward patients or clinically relevant beliefs and perceptions, though other findings were informative. For example, compared to participants with a nonmedical background, those with a medical background had significantly stronger genetic attributions for the patient’s disorder, were less confident the patient would benefit from psychotherapy, perceived the patient’s disorder as more permanent, perceived the patient to have less agency and self-control, attributed less blame to the patient, and had lower empathy and treatment self-efficacy. This study adds to the large and growing body of research on the impacts that terminology and causal explanations for substance use are important to understanding stigmatizing attitudes and recovery expectations.
For individuals and families seeking recovery: Disorders are affected by many factors including genetic attribution. This study focused on how providers’ perceptions of their patients were affected by confirming the presence of a genetic attribution. Whether a provider has a medical or non-medical background may influence their treatment approach and perception about likelihood of recovery from substance use and gambling disorders. Keep in mind that which treatment approach (medical vs non-medical) may be best is beyond the scope of this study.
For treatment professionals and treatment systems: This study found that providers with medical versus nonmedical backgrounds may respond differently to genetic attributions of disorder that can affect their beliefs about the treatment of alcohol use and gambling disorders. It is important that providers consider how their perceptions are communicated to patients and how that may impact patient behavior.
For scientists: This study focused on the impact of providing genetic explanations of alcohol and gambling disorder and how that shapes perception of providers with both medical and non-medical backgrounds. The extent to which these results generalize to interactions between family members and people with a disorder or public health messaging is unknown and should be investigated.
For policy makers: Genetic testing for substance use disorders is a tool to being used in precision medicine, which aims to understand how genes influence health and allow for customized intervention. This study examined the impact of having a genetic explanation for alcohol and gambling disorder impacted providers’ perceptions of their patients. Findings showed a genetic explanation did not affect addiction providers’ or clinicians’ attitudes toward patients or clinically relevant beliefs and perceptions. It may be that, for this group of trained addiction providers, their attitudes and beliefs were well formed based on knowledge and experience; shifting them with differing etiological explanations may be more challenging than among the general public, for example. Funding for studies that examine ideal terms and conceptual frameworks to reduce stigma toward individuals with substance use and related disorders is likely to improve individuals’ engagement with treatment and recovery supports and ultimately reduce the disease burden of alcohol and other drug use disorders.