“Street Universities”: A program for young people by young people, but do they work?
Community-based, open-door interventions are innovative approaches to engaging young people suffering from mental health and substance use challenges with pro-social activities, peers, and therapeutic services. This study described and evaluated the “Street Universities” model in Australia, which allows young people to connect with others, participate in a range of activities, and see specialized mental health professionals.
The transitions from adolescence to young adulthood correspond with many unique challenges. Yet, young people are also teeming with strengths and resiliency to overcome those challenges. Prevention and treatment research identifies the risks and protective factors of youth substance use, but few intervention or prevention strategies empower youth to voice their own opinions and make crucial health decisions. A positive youth development approach to programs and practices contends young people will thrive when programs align the strengths of young people with the resources available in their communities.
In the United States, nearly 11 million young people aged 12–25 had a substance use disorder in 2021. Yet, only about 520,000 of those individuals received any substance use treatment in that year. There are many reasons that young people may not attend or stay in treatment, including cost, access, and perceived need. In fact, 98% of adolescents believe they do not need help for their substance use. Young people could benefit from programs that provide access to mental health services if needed but also general programming that stands to enhance their holistic wellbeing, which may also indirectly benefit substance use and mental health. Non-treatment programs within the continuum of care such as adolescent peer groups (APGs) and recovery high schools (RHSs) in the US provide recovery supportive environments for adolescents in recovery from substance use, with both associated with improvements in substance use, wellbeing, and education outcomes. Similarly, recovery community centers show promise for improving outcomes for adults. Yet, empirical study of community-based supports that provide engaging activities, do not have requirements regarding recovery status to participate, and provide mental health services are significantly lacking, especially for young people across the developmental periods of adolescence and young adulthood.
Street Universities is a program that was developed in Australia in 2007 and seeks to provide community-based support for young people in disadvantaged neighborhoods. Each of the seven program locations in Australia are unique in the specific constellation of services, but they all offer workshops that leverage young people’s strengths and interests as well as mental health and education supports. The program has a mantra of “For the street, by the street,” and core elements include person-centered, low-barrier, low-threshold services, that are directly led by young people through advisory boards and ongoing feedback. Although this program has grown and is replete with anecdotal success stories, little is known about the engagement or the trajectories of young people in the therapeutic program. This study has two aims: 1) evaluate how well the program engages and retains young people and 2) assess changes in substance use, quality of life, and psychological distress among those in the optional therapeutic program.
HOW WAS THIS STUDY CONDUCTED?
The research included two separate studies focused on different yet related component parts. The first study was a prospective cohort study that followed all new program participants over a 6-month period in 2018, and it focused on retention and engagement in the overall comprehensive program. The second study was a secondary data analysis of clinical data collected over 6 years from young people who participated in the therapeutic component of the program. The secondary data analysis explored changes in substance dependence, psychological distress, and quality of life over a 90-day period.
The prospective cohort study was part of an ongoing service evaluation and featured surveys at baseline, 2, and 6 months. Participants completed the surveys on-site within 28 days of targeted timepoint and received stepped incentives for each survey ($30 Australian dollars for baseline, $40 for 2-month, and $50 for 6-month). If an individual did not return, they were sent up to four text messages inviting them to complete surveys remotely. Retention was measured by the proportion of new participants that returned after their first visit, the frequency they returned, and the average amount of time they spent at the site per visit. Those that did not return were asked to provide their primary reason for not returning. Engagement was assessed by the proportion of attendees who participated in each of the activities offered.
For the secondary data analysis, clinical data was collected as part of routine service provision in the therapeutic component of the program, which included counseling, case management, or educational interventions. Although young people could participate in these offerings as often for as long as they wished, assessments were given at regular checkpoints. Checkpoints were timed at 30-day intervals from initial intake, regardless of how frequently services were used. Intake and checkpoint assessments incorporated demographic information, drug and alcohol use including severity of dependence, psychological distress, and quality of life. Substance use frequency and severity was measured via five questions related to a self-identified primary substance of concern. The secondary data analysis only included scores from the first 90-day period after intake. Thus, some participants may have participated longer and experienced changes which are not reflected in these analyses.
There were 95 new attendees in the prospective cohort study. Among those, 60 (63%) returned for at least one additional visit within the 6-month period. The average age of those that continued to attend was 17 with a range of 14–24 years old, with just over half (57%) identifying as female. A sub-set of returning young people identified as LGBTQ (18%), Aboriginal or Torres Strait Islander (13%), and experienced recent homelessness (20%). Nearly half (43%) were currently enrolled in school. Over half (62%) reported alcohol use in the past 4 weeks, and 40% reported cannabis use in the past 4 weeks.
The routine clinical data was collected from 2014–2020 and consisted of surveys from 3,893 young people. Most (72%) were male and born in Australia (88%). There were many (40%) that received a government allowance or pension, while 21% and 29% were employed and dependent on family for income, respectively. The top three principal drugs of concern at intake were cannabis (43%), amphetamines (25%), and alcohol (21%). Nicotine (5%) benzodiazepines (2%), opioids (1%), and cocaine (1%) were also identified as principal drugs of concern for fewer young people. A small proportion (5%) were experiencing homelessness or living in supported housing, and 19% reported ever being arrested. Over half (58%) were referred to from community services (e.g., local health services, youth justices, substance use services).
WHAT DID THIS STUDY FIND?
Most young people continued to engage with program elements.
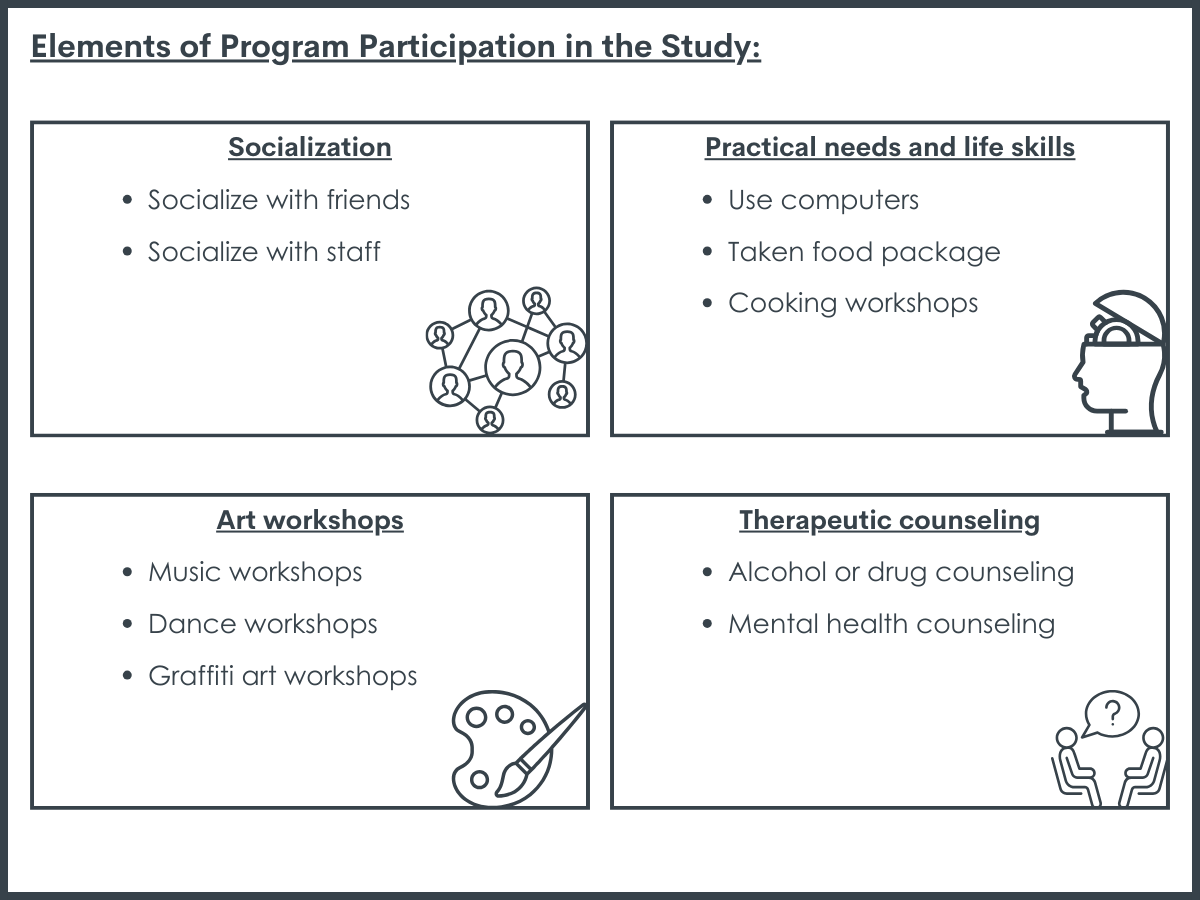
Almost two-thirds (63%) of young people returned for at least a second visit to the program during the 6-month window. Among those, 31 (54%) attended once a week or more over the 6 months. The average time spent at the site was 2.3 hours per visit. Participants engaged in a variety of services that the program offered. Socializing with friends was the most popular activity, with 89% doing so. Socializing with staff (40%) and using computers (48%) were also common activities. Participants engaged in art workshops, life skill workshops, and therapeutic counseling. There were no significant differences between those that kept attending the program and those that only attended once. Those that did not return shared the following reasons for not doing so: too busy with work, study, or family (74%), problems with transport (6%), and not feeling a need to return (20%). These reasons do suggest that youth who returned may be higher functioning and need these services less.
Young people who received therapeutic services showed improvement in outcomes.
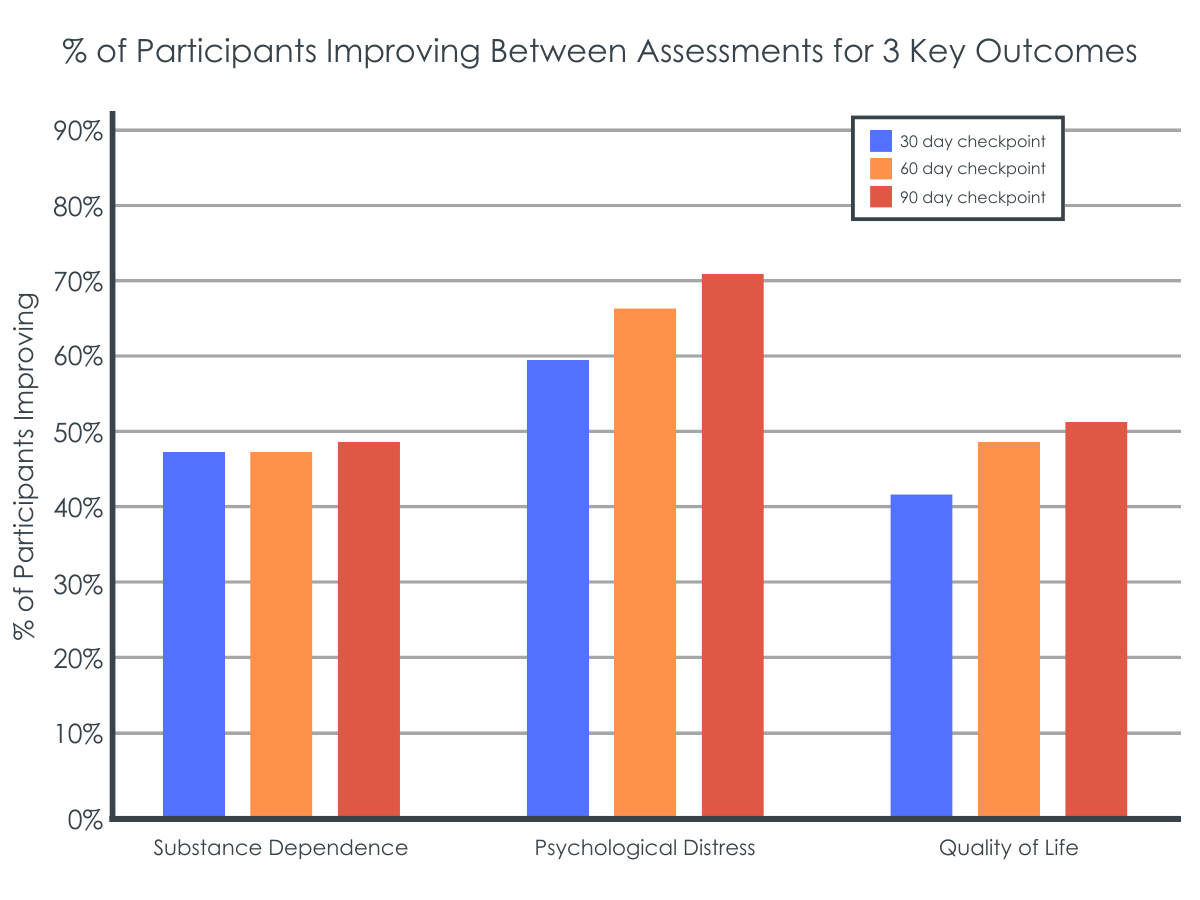
There were 1,868 (48%) young people who completed at least one 30-day post-intake checkpoint assessment in addition to their baseline assessment. There were no significant differences in age, gender, or intake scores between those that completed at least one check point assessment and those that only had a baseline assessment. Mean substance dependence severity, psychological distress, and quality of life were all reported to improve at the 30-, 60, and 90-day checkpoints. Overall, 49% of young people reduced their substance dependence, 52% experienced improved quality of life, and 71% experienced reduced distress within the 90-day study window.
Young people with most severe intake scores showed greatest improvement.
Those that had the highest level (out of three split groups) of substance dependence, psychological distress, and quality of life scores had the quickest and greatest improvement. Participants with the highest substance dependence at baseline had a 45% decrease in mean scores over the 90-day period, with the sharpest decrease occurring in the first 30 days. Those with the highest psychological distress had a 24% reduction in mean scores over the 90-day period, also with the sharpest decrease in the first 30 days. This equates to moving from “severe” distress to “moderate” distress over the study period. Participants with high and low levels of quality of life entering the program showed similar improvements over the 90-day period.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Many substance use prevention and intervention programs are regimented with specific protocols and modules. Furthermore, most programs screen participants for risk as part of the referral process or as participation criteria. There is little peer-reviewed literature surrounding community-based supports that do not require admission criteria or fees. Yet, community outreach with young people may be the most effective way of providing services for those in need.
Programs that champion youth empowerment and positive youth development may also provide a supportive environment that allows for self-led engagement and treatment planning, which may result in better outcomes than traditional programs.
The Street Universities program in Australia aims to provide young people with prosocial activities and opportunities to engage with peers in a safe and substance-free environment to build capacity, leadership, health, and wellness. In contrast to most programs, this program allows participants to self-select the frequency, duration, and ways in which they participate in general activities as well as therapeutic services such as counseling and case management. This study aimed to explore program engagement, retention, and changes in wellbeing outcomes.
The results of this study suggest that the Street Universities program in Australia retained young people in their services, and those that engaged in therapeutic services at least twice (i.e., intake and one 30-day checkpoint) typically reported improvements in substance dependence severity, psychological distress, and quality of life, at least among those who were completed a second assessment.
The young people that had the highest need, as evidenced by their worse health at baseline, showed the greatest improvements. Yet, those with better health at baseline had marginal improvements, which could suggest that the program primarily works for those struggling the most. Alternatively, those with more severe conditions also had more room to improve and may have experienced improvement without the program. Furthermore, neither the prospective cohort nor secondary data analyses were randomized control trials, nor did they include a comparison group of individuals not participating or receiving services. Thus, we are unable to say for certain that participant improvements were the result of the specific programing provided, and some of this improvement could reflect some well-known statistical “regressionto the mean” artifacts that are unrelated to the services provided.
The high retention, engagement, and general improvements in health suggest that the program may help at least some young people and is unlikely to harm them. However, more research is needed to explore what program components (e.g., life skills vs counseling) work best and for whom and over what period at what intensity of involvement. Furthermore, only 3 locations of the program were included in this study. How each community structures their Street University program and the populations they serve may result in different outcomes. How the program may scale and translate to other places, such as within rural and urban locations in in the United States, is unknown. Although more research is needed, providing young people with community-based programs to build capacity, connect with peers, and be linked to additional health services is likely to improve personal, social, and community outcomes.
This research paper incorporated two studies with two different samples. Thus, the engagement and retention outcomes cannot be linked directly with substance dependence, psychological distress, or quality of life improvements.
The severity of the primary outcomes used in the secondary data analysis are not known at the population level. We do not know the prevalence of young people in the service catchment areas struggling with substance dependence, psychological distress, or quality of life.
As mentioned above, this was not a randomized control trial, nor did it contain a comparison group of individuals not receiving services. We cannot know if those that participated in the therapeutic component of the program had improved outcomes due to the services provided or other, non-measured factors (e.g., family support, motivation to change, use of external services) or regression to the mean.
The measures used have not been validated with this age group. However, internal consistency within the study across measures is high, which suggests the measures are performing well. More work is needed to understand the best approach to measuring these key outcomes during the development periods young people traverse.
The improvements reported by the participants may not represent clinical levels of significance, meaning the improvements may not have been enough to precipitate tangible benefits for the young people. However, any improvement is hopeful and suggests future analysis and support is warranted.
The funding sustainability of community-based programs is unknown. Thus, more work is needed to understand how these programs may scale and work across communities over time.
BOTTOM LINE
The Street University program is a low-threshold, low-barrier, and person-centered intervention and prevention program for young people. The program currently has 7 locations in Australia and features 2 components: a general engagement program offering safe and fun spaces for connecting with peers, art, dance, music, and life skill workshops, and a therapeutic program that includes counselling, case management, and education intervention. This study found that in a 6-month window, 63% of new attendees returned at least once, and 54% of returnees came once a week or more over the 6 months. In a secondary analysis of clinical outcomes collected over 6 years within the therapeutic program, 49% of young people reduced their substance dependence, 52% experienced improved quality of life, and 71% experienced reduced distress within the 90-day study window. Although experimental or quasi-experimental research is needed to credit services with these improved outcomes, providing low-barrier, youth-led, and low-threshold services in the community is likely to support young people and unlikely to hamper their development.
For individuals and families seeking recovery: This study showed that young people voluntarily attended and continuing to attend a youth-led, low-barrier program providing a space to socialize, workshops ranging from cooking to graffiti, and connections to therapeutic services such as counseling. In the United States, many community-based program such as the YMCA and the Boys and Girls Club have programs geared towards young people. Additionally, programs geared directly towards young people in recovery are growing, including adolescent peer groups, recovery high schools, and recovery community centers. If you or a loved one is seeking recovery, it is likely helpful to explore local programs related directly to substance use and recovery as well as those focused on holistic health and wellness.
For treatment professionals and treatment systems: Most young people return to use within 6 months following treatment. Identifying accessible resources as part of a continuum of care is likely to benefit young people over time. This study found that young people chose to engage with a low-barrier program and that those who chose to participate in therapeutic services typically reported improvements in substance dependence, psychological distress, and quality of life over a 90-day period. Identifying available supports in the community including adolescent peer groups, recovery high schools, recovery community centers, and holistic wellness programs are likely to benefit young people leaving treatment.
For scientists: Randomized control trials are the gold standard for research and determining the impact of prevention and intervention programs. However, randomized control trails can have problems with generalizability since the participants that volunteer may not be representative of the general population. They also typically fail to capture the complexity of real-word settings. This study aimed to explore the retention, engagement, and substance use and wellbeing outcomes of a community-based program in Australia. Results indicated that young people chose to attend, with 63% returning at least once in a 6-month window. The study also found that across 6 years of clinical outcome data gathered as part of the optional therapeutic services, many young people reported improvements in substance dependence severity, psychological distress, and quality of life. Future work may work to identify how specific components or combinations of components benefit which young people and also use more naturalistic comparative effectiveness study designs in order to gauge the potential incremental benefits of using a Street University model over something else. Additionally, ongoing research can work to link how service participation is directly linked with health and wellbeing outcomes. How these programs can be scaled and developed in other locales (e.g., the United States) is also unknown and worth exploring.
For policy makers: Community-based programs that are low-barrier, low-threshold, and youth-led are uncommon, especially in the United States. Results from this study suggest that young people chose to engage in such services given the opportunity, and many young people also chose to voluntarily engage in therapeutic services like counseling, which may lead to improved personal, social, and community outcomes. Policy that supports the development of peer-designed and led community resources (e.g., recovery community centers) for young people struggling with substances is likely to enhance engagement and clinical outcomes. However, additional funding is needed to rigorously research how and for whom community resources can best support young people.
The transitions from adolescence to young adulthood correspond with many unique challenges. Yet, young people are also teeming with strengths and resiliency to overcome those challenges. Prevention and treatment research identifies the risks and protective factors of youth substance use, but few intervention or prevention strategies empower youth to voice their own opinions and make crucial health decisions. A positive youth development approach to programs and practices contends young people will thrive when programs align the strengths of young people with the resources available in their communities.
In the United States, nearly 11 million young people aged 12–25 had a substance use disorder in 2021. Yet, only about 520,000 of those individuals received any substance use treatment in that year. There are many reasons that young people may not attend or stay in treatment, including cost, access, and perceived need. In fact, 98% of adolescents believe they do not need help for their substance use. Young people could benefit from programs that provide access to mental health services if needed but also general programming that stands to enhance their holistic wellbeing, which may also indirectly benefit substance use and mental health. Non-treatment programs within the continuum of care such as adolescent peer groups (APGs) and recovery high schools (RHSs) in the US provide recovery supportive environments for adolescents in recovery from substance use, with both associated with improvements in substance use, wellbeing, and education outcomes. Similarly, recovery community centers show promise for improving outcomes for adults. Yet, empirical study of community-based supports that provide engaging activities, do not have requirements regarding recovery status to participate, and provide mental health services are significantly lacking, especially for young people across the developmental periods of adolescence and young adulthood.
Street Universities is a program that was developed in Australia in 2007 and seeks to provide community-based support for young people in disadvantaged neighborhoods. Each of the seven program locations in Australia are unique in the specific constellation of services, but they all offer workshops that leverage young people’s strengths and interests as well as mental health and education supports. The program has a mantra of “For the street, by the street,” and core elements include person-centered, low-barrier, low-threshold services, that are directly led by young people through advisory boards and ongoing feedback. Although this program has grown and is replete with anecdotal success stories, little is known about the engagement or the trajectories of young people in the therapeutic program. This study has two aims: 1) evaluate how well the program engages and retains young people and 2) assess changes in substance use, quality of life, and psychological distress among those in the optional therapeutic program.
HOW WAS THIS STUDY CONDUCTED?
The research included two separate studies focused on different yet related component parts. The first study was a prospective cohort study that followed all new program participants over a 6-month period in 2018, and it focused on retention and engagement in the overall comprehensive program. The second study was a secondary data analysis of clinical data collected over 6 years from young people who participated in the therapeutic component of the program. The secondary data analysis explored changes in substance dependence, psychological distress, and quality of life over a 90-day period.
The prospective cohort study was part of an ongoing service evaluation and featured surveys at baseline, 2, and 6 months. Participants completed the surveys on-site within 28 days of targeted timepoint and received stepped incentives for each survey ($30 Australian dollars for baseline, $40 for 2-month, and $50 for 6-month). If an individual did not return, they were sent up to four text messages inviting them to complete surveys remotely. Retention was measured by the proportion of new participants that returned after their first visit, the frequency they returned, and the average amount of time they spent at the site per visit. Those that did not return were asked to provide their primary reason for not returning. Engagement was assessed by the proportion of attendees who participated in each of the activities offered.
For the secondary data analysis, clinical data was collected as part of routine service provision in the therapeutic component of the program, which included counseling, case management, or educational interventions. Although young people could participate in these offerings as often for as long as they wished, assessments were given at regular checkpoints. Checkpoints were timed at 30-day intervals from initial intake, regardless of how frequently services were used. Intake and checkpoint assessments incorporated demographic information, drug and alcohol use including severity of dependence, psychological distress, and quality of life. Substance use frequency and severity was measured via five questions related to a self-identified primary substance of concern. The secondary data analysis only included scores from the first 90-day period after intake. Thus, some participants may have participated longer and experienced changes which are not reflected in these analyses.
There were 95 new attendees in the prospective cohort study. Among those, 60 (63%) returned for at least one additional visit within the 6-month period. The average age of those that continued to attend was 17 with a range of 14–24 years old, with just over half (57%) identifying as female. A sub-set of returning young people identified as LGBTQ (18%), Aboriginal or Torres Strait Islander (13%), and experienced recent homelessness (20%). Nearly half (43%) were currently enrolled in school. Over half (62%) reported alcohol use in the past 4 weeks, and 40% reported cannabis use in the past 4 weeks.
The routine clinical data was collected from 2014–2020 and consisted of surveys from 3,893 young people. Most (72%) were male and born in Australia (88%). There were many (40%) that received a government allowance or pension, while 21% and 29% were employed and dependent on family for income, respectively. The top three principal drugs of concern at intake were cannabis (43%), amphetamines (25%), and alcohol (21%). Nicotine (5%) benzodiazepines (2%), opioids (1%), and cocaine (1%) were also identified as principal drugs of concern for fewer young people. A small proportion (5%) were experiencing homelessness or living in supported housing, and 19% reported ever being arrested. Over half (58%) were referred to from community services (e.g., local health services, youth justices, substance use services).
WHAT DID THIS STUDY FIND?
Most young people continued to engage with program elements.
Almost two-thirds (63%) of young people returned for at least a second visit to the program during the 6-month window. Among those, 31 (54%) attended once a week or more over the 6 months. The average time spent at the site was 2.3 hours per visit. Participants engaged in a variety of services that the program offered. Socializing with friends was the most popular activity, with 89% doing so. Socializing with staff (40%) and using computers (48%) were also common activities. Participants engaged in art workshops, life skill workshops, and therapeutic counseling. There were no significant differences between those that kept attending the program and those that only attended once. Those that did not return shared the following reasons for not doing so: too busy with work, study, or family (74%), problems with transport (6%), and not feeling a need to return (20%). These reasons do suggest that youth who returned may be higher functioning and need these services less.
Young people who received therapeutic services showed improvement in outcomes.
There were 1,868 (48%) young people who completed at least one 30-day post-intake checkpoint assessment in addition to their baseline assessment. There were no significant differences in age, gender, or intake scores between those that completed at least one check point assessment and those that only had a baseline assessment. Mean substance dependence severity, psychological distress, and quality of life were all reported to improve at the 30-, 60, and 90-day checkpoints. Overall, 49% of young people reduced their substance dependence, 52% experienced improved quality of life, and 71% experienced reduced distress within the 90-day study window.
Young people with most severe intake scores showed greatest improvement.
Those that had the highest level (out of three split groups) of substance dependence, psychological distress, and quality of life scores had the quickest and greatest improvement. Participants with the highest substance dependence at baseline had a 45% decrease in mean scores over the 90-day period, with the sharpest decrease occurring in the first 30 days. Those with the highest psychological distress had a 24% reduction in mean scores over the 90-day period, also with the sharpest decrease in the first 30 days. This equates to moving from “severe” distress to “moderate” distress over the study period. Participants with high and low levels of quality of life entering the program showed similar improvements over the 90-day period.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Many substance use prevention and intervention programs are regimented with specific protocols and modules. Furthermore, most programs screen participants for risk as part of the referral process or as participation criteria. There is little peer-reviewed literature surrounding community-based supports that do not require admission criteria or fees. Yet, community outreach with young people may be the most effective way of providing services for those in need.
Programs that champion youth empowerment and positive youth development may also provide a supportive environment that allows for self-led engagement and treatment planning, which may result in better outcomes than traditional programs.
The Street Universities program in Australia aims to provide young people with prosocial activities and opportunities to engage with peers in a safe and substance-free environment to build capacity, leadership, health, and wellness. In contrast to most programs, this program allows participants to self-select the frequency, duration, and ways in which they participate in general activities as well as therapeutic services such as counseling and case management. This study aimed to explore program engagement, retention, and changes in wellbeing outcomes.
The results of this study suggest that the Street Universities program in Australia retained young people in their services, and those that engaged in therapeutic services at least twice (i.e., intake and one 30-day checkpoint) typically reported improvements in substance dependence severity, psychological distress, and quality of life, at least among those who were completed a second assessment.
The young people that had the highest need, as evidenced by their worse health at baseline, showed the greatest improvements. Yet, those with better health at baseline had marginal improvements, which could suggest that the program primarily works for those struggling the most. Alternatively, those with more severe conditions also had more room to improve and may have experienced improvement without the program. Furthermore, neither the prospective cohort nor secondary data analyses were randomized control trials, nor did they include a comparison group of individuals not participating or receiving services. Thus, we are unable to say for certain that participant improvements were the result of the specific programing provided, and some of this improvement could reflect some well-known statistical “regressionto the mean” artifacts that are unrelated to the services provided.
The high retention, engagement, and general improvements in health suggest that the program may help at least some young people and is unlikely to harm them. However, more research is needed to explore what program components (e.g., life skills vs counseling) work best and for whom and over what period at what intensity of involvement. Furthermore, only 3 locations of the program were included in this study. How each community structures their Street University program and the populations they serve may result in different outcomes. How the program may scale and translate to other places, such as within rural and urban locations in in the United States, is unknown. Although more research is needed, providing young people with community-based programs to build capacity, connect with peers, and be linked to additional health services is likely to improve personal, social, and community outcomes.
This research paper incorporated two studies with two different samples. Thus, the engagement and retention outcomes cannot be linked directly with substance dependence, psychological distress, or quality of life improvements.
The severity of the primary outcomes used in the secondary data analysis are not known at the population level. We do not know the prevalence of young people in the service catchment areas struggling with substance dependence, psychological distress, or quality of life.
As mentioned above, this was not a randomized control trial, nor did it contain a comparison group of individuals not receiving services. We cannot know if those that participated in the therapeutic component of the program had improved outcomes due to the services provided or other, non-measured factors (e.g., family support, motivation to change, use of external services) or regression to the mean.
The measures used have not been validated with this age group. However, internal consistency within the study across measures is high, which suggests the measures are performing well. More work is needed to understand the best approach to measuring these key outcomes during the development periods young people traverse.
The improvements reported by the participants may not represent clinical levels of significance, meaning the improvements may not have been enough to precipitate tangible benefits for the young people. However, any improvement is hopeful and suggests future analysis and support is warranted.
The funding sustainability of community-based programs is unknown. Thus, more work is needed to understand how these programs may scale and work across communities over time.
BOTTOM LINE
The Street University program is a low-threshold, low-barrier, and person-centered intervention and prevention program for young people. The program currently has 7 locations in Australia and features 2 components: a general engagement program offering safe and fun spaces for connecting with peers, art, dance, music, and life skill workshops, and a therapeutic program that includes counselling, case management, and education intervention. This study found that in a 6-month window, 63% of new attendees returned at least once, and 54% of returnees came once a week or more over the 6 months. In a secondary analysis of clinical outcomes collected over 6 years within the therapeutic program, 49% of young people reduced their substance dependence, 52% experienced improved quality of life, and 71% experienced reduced distress within the 90-day study window. Although experimental or quasi-experimental research is needed to credit services with these improved outcomes, providing low-barrier, youth-led, and low-threshold services in the community is likely to support young people and unlikely to hamper their development.
For individuals and families seeking recovery: This study showed that young people voluntarily attended and continuing to attend a youth-led, low-barrier program providing a space to socialize, workshops ranging from cooking to graffiti, and connections to therapeutic services such as counseling. In the United States, many community-based program such as the YMCA and the Boys and Girls Club have programs geared towards young people. Additionally, programs geared directly towards young people in recovery are growing, including adolescent peer groups, recovery high schools, and recovery community centers. If you or a loved one is seeking recovery, it is likely helpful to explore local programs related directly to substance use and recovery as well as those focused on holistic health and wellness.
For treatment professionals and treatment systems: Most young people return to use within 6 months following treatment. Identifying accessible resources as part of a continuum of care is likely to benefit young people over time. This study found that young people chose to engage with a low-barrier program and that those who chose to participate in therapeutic services typically reported improvements in substance dependence, psychological distress, and quality of life over a 90-day period. Identifying available supports in the community including adolescent peer groups, recovery high schools, recovery community centers, and holistic wellness programs are likely to benefit young people leaving treatment.
For scientists: Randomized control trials are the gold standard for research and determining the impact of prevention and intervention programs. However, randomized control trails can have problems with generalizability since the participants that volunteer may not be representative of the general population. They also typically fail to capture the complexity of real-word settings. This study aimed to explore the retention, engagement, and substance use and wellbeing outcomes of a community-based program in Australia. Results indicated that young people chose to attend, with 63% returning at least once in a 6-month window. The study also found that across 6 years of clinical outcome data gathered as part of the optional therapeutic services, many young people reported improvements in substance dependence severity, psychological distress, and quality of life. Future work may work to identify how specific components or combinations of components benefit which young people and also use more naturalistic comparative effectiveness study designs in order to gauge the potential incremental benefits of using a Street University model over something else. Additionally, ongoing research can work to link how service participation is directly linked with health and wellbeing outcomes. How these programs can be scaled and developed in other locales (e.g., the United States) is also unknown and worth exploring.
For policy makers: Community-based programs that are low-barrier, low-threshold, and youth-led are uncommon, especially in the United States. Results from this study suggest that young people chose to engage in such services given the opportunity, and many young people also chose to voluntarily engage in therapeutic services like counseling, which may lead to improved personal, social, and community outcomes. Policy that supports the development of peer-designed and led community resources (e.g., recovery community centers) for young people struggling with substances is likely to enhance engagement and clinical outcomes. However, additional funding is needed to rigorously research how and for whom community resources can best support young people.
The transitions from adolescence to young adulthood correspond with many unique challenges. Yet, young people are also teeming with strengths and resiliency to overcome those challenges. Prevention and treatment research identifies the risks and protective factors of youth substance use, but few intervention or prevention strategies empower youth to voice their own opinions and make crucial health decisions. A positive youth development approach to programs and practices contends young people will thrive when programs align the strengths of young people with the resources available in their communities.
In the United States, nearly 11 million young people aged 12–25 had a substance use disorder in 2021. Yet, only about 520,000 of those individuals received any substance use treatment in that year. There are many reasons that young people may not attend or stay in treatment, including cost, access, and perceived need. In fact, 98% of adolescents believe they do not need help for their substance use. Young people could benefit from programs that provide access to mental health services if needed but also general programming that stands to enhance their holistic wellbeing, which may also indirectly benefit substance use and mental health. Non-treatment programs within the continuum of care such as adolescent peer groups (APGs) and recovery high schools (RHSs) in the US provide recovery supportive environments for adolescents in recovery from substance use, with both associated with improvements in substance use, wellbeing, and education outcomes. Similarly, recovery community centers show promise for improving outcomes for adults. Yet, empirical study of community-based supports that provide engaging activities, do not have requirements regarding recovery status to participate, and provide mental health services are significantly lacking, especially for young people across the developmental periods of adolescence and young adulthood.
Street Universities is a program that was developed in Australia in 2007 and seeks to provide community-based support for young people in disadvantaged neighborhoods. Each of the seven program locations in Australia are unique in the specific constellation of services, but they all offer workshops that leverage young people’s strengths and interests as well as mental health and education supports. The program has a mantra of “For the street, by the street,” and core elements include person-centered, low-barrier, low-threshold services, that are directly led by young people through advisory boards and ongoing feedback. Although this program has grown and is replete with anecdotal success stories, little is known about the engagement or the trajectories of young people in the therapeutic program. This study has two aims: 1) evaluate how well the program engages and retains young people and 2) assess changes in substance use, quality of life, and psychological distress among those in the optional therapeutic program.
HOW WAS THIS STUDY CONDUCTED?
The research included two separate studies focused on different yet related component parts. The first study was a prospective cohort study that followed all new program participants over a 6-month period in 2018, and it focused on retention and engagement in the overall comprehensive program. The second study was a secondary data analysis of clinical data collected over 6 years from young people who participated in the therapeutic component of the program. The secondary data analysis explored changes in substance dependence, psychological distress, and quality of life over a 90-day period.
The prospective cohort study was part of an ongoing service evaluation and featured surveys at baseline, 2, and 6 months. Participants completed the surveys on-site within 28 days of targeted timepoint and received stepped incentives for each survey ($30 Australian dollars for baseline, $40 for 2-month, and $50 for 6-month). If an individual did not return, they were sent up to four text messages inviting them to complete surveys remotely. Retention was measured by the proportion of new participants that returned after their first visit, the frequency they returned, and the average amount of time they spent at the site per visit. Those that did not return were asked to provide their primary reason for not returning. Engagement was assessed by the proportion of attendees who participated in each of the activities offered.
For the secondary data analysis, clinical data was collected as part of routine service provision in the therapeutic component of the program, which included counseling, case management, or educational interventions. Although young people could participate in these offerings as often for as long as they wished, assessments were given at regular checkpoints. Checkpoints were timed at 30-day intervals from initial intake, regardless of how frequently services were used. Intake and checkpoint assessments incorporated demographic information, drug and alcohol use including severity of dependence, psychological distress, and quality of life. Substance use frequency and severity was measured via five questions related to a self-identified primary substance of concern. The secondary data analysis only included scores from the first 90-day period after intake. Thus, some participants may have participated longer and experienced changes which are not reflected in these analyses.
There were 95 new attendees in the prospective cohort study. Among those, 60 (63%) returned for at least one additional visit within the 6-month period. The average age of those that continued to attend was 17 with a range of 14–24 years old, with just over half (57%) identifying as female. A sub-set of returning young people identified as LGBTQ (18%), Aboriginal or Torres Strait Islander (13%), and experienced recent homelessness (20%). Nearly half (43%) were currently enrolled in school. Over half (62%) reported alcohol use in the past 4 weeks, and 40% reported cannabis use in the past 4 weeks.
The routine clinical data was collected from 2014–2020 and consisted of surveys from 3,893 young people. Most (72%) were male and born in Australia (88%). There were many (40%) that received a government allowance or pension, while 21% and 29% were employed and dependent on family for income, respectively. The top three principal drugs of concern at intake were cannabis (43%), amphetamines (25%), and alcohol (21%). Nicotine (5%) benzodiazepines (2%), opioids (1%), and cocaine (1%) were also identified as principal drugs of concern for fewer young people. A small proportion (5%) were experiencing homelessness or living in supported housing, and 19% reported ever being arrested. Over half (58%) were referred to from community services (e.g., local health services, youth justices, substance use services).
WHAT DID THIS STUDY FIND?
Most young people continued to engage with program elements.
Almost two-thirds (63%) of young people returned for at least a second visit to the program during the 6-month window. Among those, 31 (54%) attended once a week or more over the 6 months. The average time spent at the site was 2.3 hours per visit. Participants engaged in a variety of services that the program offered. Socializing with friends was the most popular activity, with 89% doing so. Socializing with staff (40%) and using computers (48%) were also common activities. Participants engaged in art workshops, life skill workshops, and therapeutic counseling. There were no significant differences between those that kept attending the program and those that only attended once. Those that did not return shared the following reasons for not doing so: too busy with work, study, or family (74%), problems with transport (6%), and not feeling a need to return (20%). These reasons do suggest that youth who returned may be higher functioning and need these services less.
Young people who received therapeutic services showed improvement in outcomes.
There were 1,868 (48%) young people who completed at least one 30-day post-intake checkpoint assessment in addition to their baseline assessment. There were no significant differences in age, gender, or intake scores between those that completed at least one check point assessment and those that only had a baseline assessment. Mean substance dependence severity, psychological distress, and quality of life were all reported to improve at the 30-, 60, and 90-day checkpoints. Overall, 49% of young people reduced their substance dependence, 52% experienced improved quality of life, and 71% experienced reduced distress within the 90-day study window.
Young people with most severe intake scores showed greatest improvement.
Those that had the highest level (out of three split groups) of substance dependence, psychological distress, and quality of life scores had the quickest and greatest improvement. Participants with the highest substance dependence at baseline had a 45% decrease in mean scores over the 90-day period, with the sharpest decrease occurring in the first 30 days. Those with the highest psychological distress had a 24% reduction in mean scores over the 90-day period, also with the sharpest decrease in the first 30 days. This equates to moving from “severe” distress to “moderate” distress over the study period. Participants with high and low levels of quality of life entering the program showed similar improvements over the 90-day period.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Many substance use prevention and intervention programs are regimented with specific protocols and modules. Furthermore, most programs screen participants for risk as part of the referral process or as participation criteria. There is little peer-reviewed literature surrounding community-based supports that do not require admission criteria or fees. Yet, community outreach with young people may be the most effective way of providing services for those in need.
Programs that champion youth empowerment and positive youth development may also provide a supportive environment that allows for self-led engagement and treatment planning, which may result in better outcomes than traditional programs.
The Street Universities program in Australia aims to provide young people with prosocial activities and opportunities to engage with peers in a safe and substance-free environment to build capacity, leadership, health, and wellness. In contrast to most programs, this program allows participants to self-select the frequency, duration, and ways in which they participate in general activities as well as therapeutic services such as counseling and case management. This study aimed to explore program engagement, retention, and changes in wellbeing outcomes.
The results of this study suggest that the Street Universities program in Australia retained young people in their services, and those that engaged in therapeutic services at least twice (i.e., intake and one 30-day checkpoint) typically reported improvements in substance dependence severity, psychological distress, and quality of life, at least among those who were completed a second assessment.
The young people that had the highest need, as evidenced by their worse health at baseline, showed the greatest improvements. Yet, those with better health at baseline had marginal improvements, which could suggest that the program primarily works for those struggling the most. Alternatively, those with more severe conditions also had more room to improve and may have experienced improvement without the program. Furthermore, neither the prospective cohort nor secondary data analyses were randomized control trials, nor did they include a comparison group of individuals not participating or receiving services. Thus, we are unable to say for certain that participant improvements were the result of the specific programing provided, and some of this improvement could reflect some well-known statistical “regressionto the mean” artifacts that are unrelated to the services provided.
The high retention, engagement, and general improvements in health suggest that the program may help at least some young people and is unlikely to harm them. However, more research is needed to explore what program components (e.g., life skills vs counseling) work best and for whom and over what period at what intensity of involvement. Furthermore, only 3 locations of the program were included in this study. How each community structures their Street University program and the populations they serve may result in different outcomes. How the program may scale and translate to other places, such as within rural and urban locations in in the United States, is unknown. Although more research is needed, providing young people with community-based programs to build capacity, connect with peers, and be linked to additional health services is likely to improve personal, social, and community outcomes.
This research paper incorporated two studies with two different samples. Thus, the engagement and retention outcomes cannot be linked directly with substance dependence, psychological distress, or quality of life improvements.
The severity of the primary outcomes used in the secondary data analysis are not known at the population level. We do not know the prevalence of young people in the service catchment areas struggling with substance dependence, psychological distress, or quality of life.
As mentioned above, this was not a randomized control trial, nor did it contain a comparison group of individuals not receiving services. We cannot know if those that participated in the therapeutic component of the program had improved outcomes due to the services provided or other, non-measured factors (e.g., family support, motivation to change, use of external services) or regression to the mean.
The measures used have not been validated with this age group. However, internal consistency within the study across measures is high, which suggests the measures are performing well. More work is needed to understand the best approach to measuring these key outcomes during the development periods young people traverse.
The improvements reported by the participants may not represent clinical levels of significance, meaning the improvements may not have been enough to precipitate tangible benefits for the young people. However, any improvement is hopeful and suggests future analysis and support is warranted.
The funding sustainability of community-based programs is unknown. Thus, more work is needed to understand how these programs may scale and work across communities over time.
BOTTOM LINE
The Street University program is a low-threshold, low-barrier, and person-centered intervention and prevention program for young people. The program currently has 7 locations in Australia and features 2 components: a general engagement program offering safe and fun spaces for connecting with peers, art, dance, music, and life skill workshops, and a therapeutic program that includes counselling, case management, and education intervention. This study found that in a 6-month window, 63% of new attendees returned at least once, and 54% of returnees came once a week or more over the 6 months. In a secondary analysis of clinical outcomes collected over 6 years within the therapeutic program, 49% of young people reduced their substance dependence, 52% experienced improved quality of life, and 71% experienced reduced distress within the 90-day study window. Although experimental or quasi-experimental research is needed to credit services with these improved outcomes, providing low-barrier, youth-led, and low-threshold services in the community is likely to support young people and unlikely to hamper their development.
For individuals and families seeking recovery: This study showed that young people voluntarily attended and continuing to attend a youth-led, low-barrier program providing a space to socialize, workshops ranging from cooking to graffiti, and connections to therapeutic services such as counseling. In the United States, many community-based program such as the YMCA and the Boys and Girls Club have programs geared towards young people. Additionally, programs geared directly towards young people in recovery are growing, including adolescent peer groups, recovery high schools, and recovery community centers. If you or a loved one is seeking recovery, it is likely helpful to explore local programs related directly to substance use and recovery as well as those focused on holistic health and wellness.
For treatment professionals and treatment systems: Most young people return to use within 6 months following treatment. Identifying accessible resources as part of a continuum of care is likely to benefit young people over time. This study found that young people chose to engage with a low-barrier program and that those who chose to participate in therapeutic services typically reported improvements in substance dependence, psychological distress, and quality of life over a 90-day period. Identifying available supports in the community including adolescent peer groups, recovery high schools, recovery community centers, and holistic wellness programs are likely to benefit young people leaving treatment.
For scientists: Randomized control trials are the gold standard for research and determining the impact of prevention and intervention programs. However, randomized control trails can have problems with generalizability since the participants that volunteer may not be representative of the general population. They also typically fail to capture the complexity of real-word settings. This study aimed to explore the retention, engagement, and substance use and wellbeing outcomes of a community-based program in Australia. Results indicated that young people chose to attend, with 63% returning at least once in a 6-month window. The study also found that across 6 years of clinical outcome data gathered as part of the optional therapeutic services, many young people reported improvements in substance dependence severity, psychological distress, and quality of life. Future work may work to identify how specific components or combinations of components benefit which young people and also use more naturalistic comparative effectiveness study designs in order to gauge the potential incremental benefits of using a Street University model over something else. Additionally, ongoing research can work to link how service participation is directly linked with health and wellbeing outcomes. How these programs can be scaled and developed in other locales (e.g., the United States) is also unknown and worth exploring.
For policy makers: Community-based programs that are low-barrier, low-threshold, and youth-led are uncommon, especially in the United States. Results from this study suggest that young people chose to engage in such services given the opportunity, and many young people also chose to voluntarily engage in therapeutic services like counseling, which may lead to improved personal, social, and community outcomes. Policy that supports the development of peer-designed and led community resources (e.g., recovery community centers) for young people struggling with substances is likely to enhance engagement and clinical outcomes. However, additional funding is needed to rigorously research how and for whom community resources can best support young people.