Testing the active ingredients of motivational interviewing to reduce alcohol use: Things are not quite what they seem
Motivational interviewing is a popular, widely used, talk therapy to enhance motivation to change a behavior, such as cutting down or quitting alcohol or other drug use. Despite its wide use, researchers and clinicians do not know what components of motivational interviewing are essential – in other words, what makes the therapy work. This study tested two versions of motivational interviewing against a no treatment group to identify the essential ingredients needed to effect behavior change.
Motivational Interviewing (MI), sometimes packaged in a manualized treatment called Motivational Enhancement Therapy (MET), is a widely used counseling approach to resolve ambivalence and enhance motivation to change a behavior. It is most commonly known for its use in alcohol and other drug use treatment and has been used in other health contexts such as smoking cessation, diet and exercise, and HIV risk reduction. Compared to no intervention, or a non-therapy-based intervention (e.g., assessment only or waitlist control), MI has strong empirical support, though it does not do any better than other kinds of interventions.
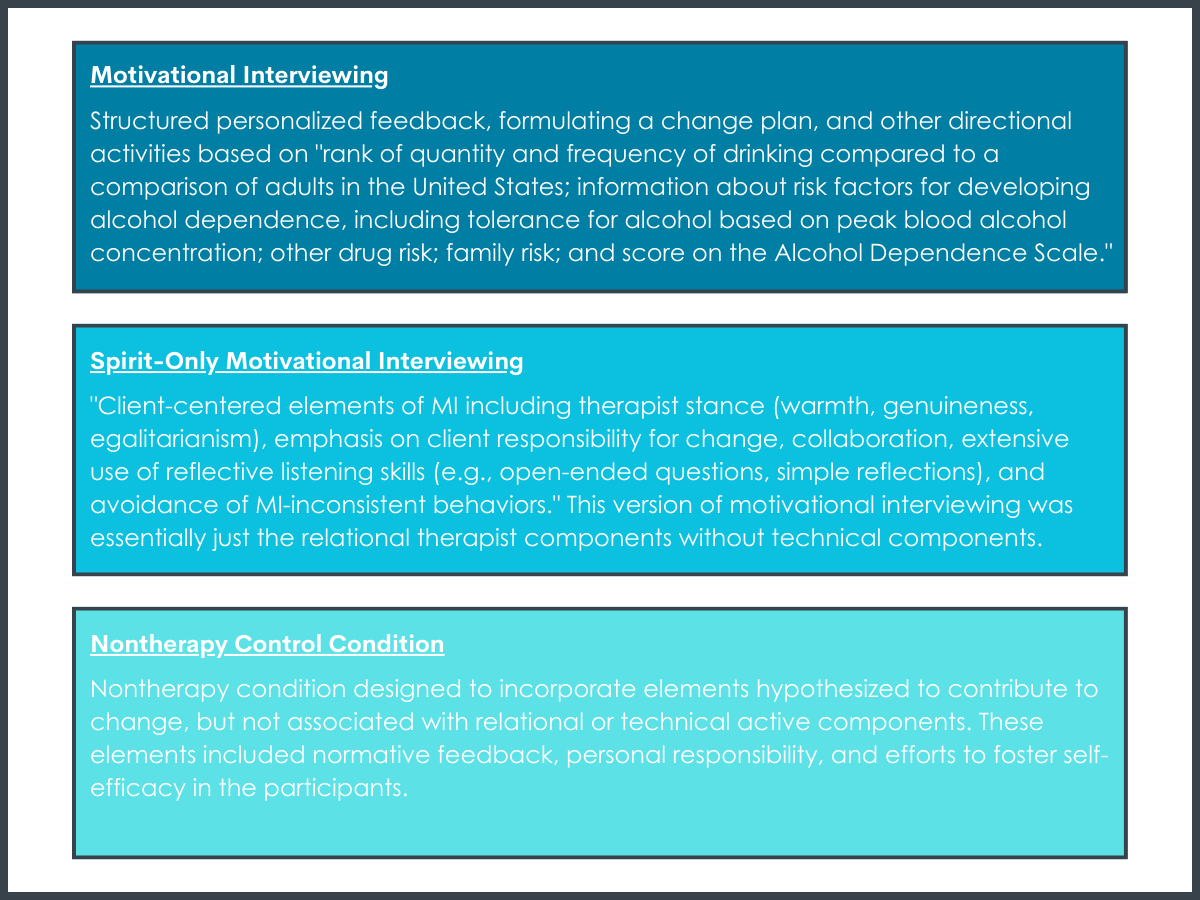
MI is often delivered as a brief intervention based on client-centered principles, including autonomy and self-determination, support, and positive regard, and emphasizes common counseling skills such as reflective listening, accurate empathy, expressing acceptance of the patient’s goals, and affirmation of the patient’s freedom of choice.
These client-centered principles are sometimes referred to as the “spirit of MI” or the “relational” components of MI. This approach, however, also employs strategies such as selective reinforcement of talk focused on behavior change (“change talk”) and helping the patient realize discrepancies between their values or goals and their actual behavior. These more “directional” strategies are sometimes referred to as the “technical” components of MI. Both “relational” and “technical” components of MI are thought to be necessary to affect behavior change, however research thus far has limited support for either theory. For example, in a meta-analysis of studies that examined the “relational” and “technical” components of MI, the more therapists’ counseling skills were consistent with MI relational and technical components, the more a patient verbalized “change talk” in the counseling session(s). However, the amount patients verbalized “change talk” in the counseling session(s) did not predict their changes in drinking, thus not supporting the presumed theoretical mechanism of how the therapy works.
To try to elucidate what in MI is actually making the difference, this study employed a “dismantling” randomized clinical trial design to pinpoint empirical support for the relational or technical components of MI, by comparing three therapy conditions: Full MI vs spirit-only MI vs non-therapy brief advice. The researchers of this study had conducted a similar study prior that showed no benefit of MI over the non-therapy brief advice. This study addresses limitations of that prior study, including the smaller sample sizes in the prior study, and tests if results could be replicated and are robust. Furthermore, because MI is meant to enhance motivation, the researchers wanted to know if MI would be more helpful for participants who started with lower motivation to reduce drinking than if they had received brief advice and no therapy.
HOW WAS THIS STUDY CONDUCTED?
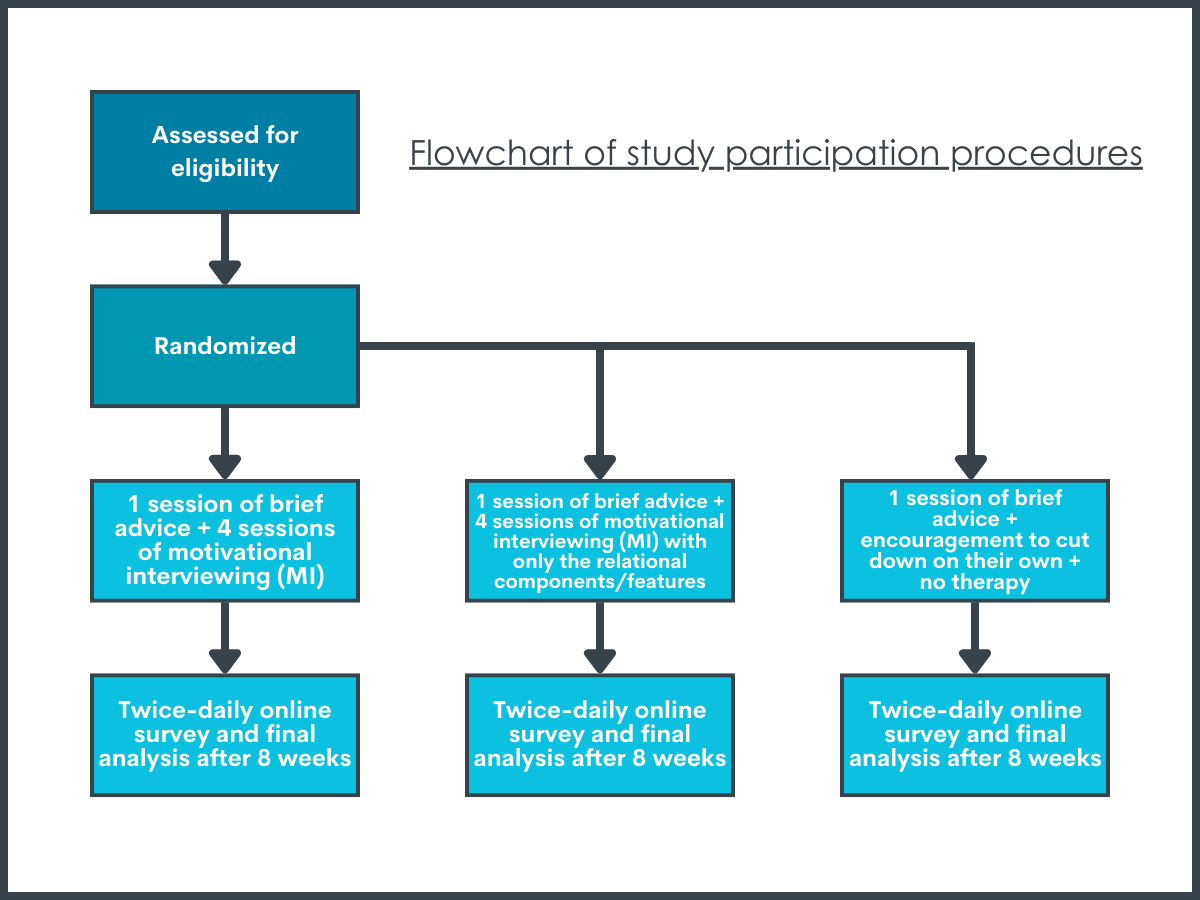
This randomized clinical trial used a dismantling study design to examine the effects of Motivational Interviewing (MI) on drinking outcomes over 8 weeks among 139 adults seeking help to reduce (but not necessarily abstain from) drinking. Adults seeking to reduce drinking were randomly assigned to receive either:
1 session of brief advice + 4 sessions of motivational interviewing (MI) with all of the standard MI components/features included, called “MI”
1 session of brief advice + 4 sessions of motivational interviewing (MI) with only the relational components/features (without the technical components), called “spirit-only MI”
1 session of brief advice + encouragement to cut down on their own + no therapy
All participants were asked to respond to a twice-daily online survey that included daily reports on their drinking over the 8-week study period.
Participants were recruited via advertisements online and in local media emphasizing a primary goal of reduced drinking (i.e., not abstinence). Interested adults were initially assessed for eligibility using valid and commonly used screeners for alcohol and other drug use, other psychiatric disorders, and cognitive functioning. Participants were included in the study if they were (a) between the ages of 18 and 75, (b) in the past 2 months, drank an average of 15+ drinks per week for women or 24+ drinks per week for men, and (c) met criteria for an Alcohol Use Disorder. Adults were not eligible to participate if they (a) met criteria for another substance use disorder (other than alcohol, cannabis, or nicotine) or used other drugs 2+ times weekly, (b) presented with a serious psychiatric disorder or suicide or violence risk at time of eligibility assessment, (c) had a history of serious alcohol withdrawal symptoms, such as seizures, (d) were legally mandated to substance use treatment, (e) reported social instability (e.g., unstable housing), (f) expressed a desire at eligibility screening to achieve abstinence, or (g) expressed a desire or intent to obtain additional substance use treatment during the 8-week treatment period.
After confirming eligibility, participants were texted twice a day to respond to an online survey asking, “Did you drink yesterday since your morning survey?” When participants responded “yes” to this question, they were asked to report the number of standard drinks of beer, wine, and liquor that they had consumed in the last 24 hours. Participants were also asked about their level of motivation to cut down: “How committed are you to not drink heavily (that is, drink 4 or more drinks for women, 5 or more drinks for men) in the next 24 hours?” Response options ranged from 0 (not at all) to 8 (extremely). Participants received these prompts for the first 2 weeks of the study (i.e., for 1 week after eligibility screening but prior to baseline assessment and randomization to treatment and 1 week following baseline assessment/randomization), as well as during weeks 4 and 7 for a total of 28 days of surveys during the study period.
This daily survey method (called Ecological Momentary Assessment or “EMA”) is meant to get real time, “in the moment” information or with minimal time between the survey and the event, which may be more accurate than asking participants to recall their drinking over a longer period (e.g., past month or more). This frequent assessment may also serve as a form of self-monitoring. Self-monitoring is a commonly used technique when trying to make improvements to a health behavior, such as tracking your steps or keeping a food journal. Bringing greater awareness to a particular behavior alone may change or improve that behavior. Because of this potential therapeutic effect, the researchers started the twice-daily messages 1 week early to test if the twice-daily surveys would influence participants drinking on its own.
After 1 week of twice-daily surveys, participants returned to complete baseline assessment and randomized to receive one of three treatments. During the baseline assessment, participants answered questions about their level of motivation to cut down their drinking (sometimes referred to as “stages of change”) using a psychometrically valid 12-item questionnaire, and completed an interview with a research assistant to record their drinking from the past 8 weeks.
All participants received feedback (brief advice) from a research assistant on their estimated average drinks per week and risk level based on commonly used alcohol use disorder screening measures (low risk, excess of low risk, harmful/hazardous risk, or may be physically dependent) during the baseline assessment. Then participants were randomized to intervention condition. MI and spirit-only MI were both delivered in four sessions that lasted between 45-60 minutes at weeks 1, 2, 5, and 8. Participants randomized to the “no therapy” condition were encouraged to cut down on their own and received no additional treatment.
Recordings of MI and spirit-only MI sessions were reviewed to ensure the study counselors adhered to the specific components of MI intended for the different treatments. Because the study compares different components of MI, it was important for the researchers to ensure that MI and the spirit-only MI were closely following those specific counseling skills and techniques, and that the types of counseling were different from each other. To show this, MI and spirit-only MI sessions were coded with a commonly used MI-specific coding scheme that identifies the specific relational and technical counseling techniques.
In terms of drinking outcomes, first, the analysis tested if there were reductions in drinking over the 8-week study period, and if the treatments were associated with different reductions in alcohol use, controlling for baseline level of use and relevant demographic and clinical characteristics (age, gender, educational and occupational information, race and ethnicity, medical history, family psychiatric and substance abuse history, and the participant’s substance use treatment history). Second, the analysis tested if motivation to change alcohol use was associated with actual reductions in use, and if specific treatments worked better for reducing alcohol use depending on level of motivation. Since MI is meant to enhance motivation, the researchers predicted that the full MI might be more helpful in reducing drinking for participants with low motivation, than participants with higher motivation or other treatment types. The researchers examined both motivation to change at baseline, as well as motivation over time throughout the study from the twice-daily survey.
Participants were mostly middle-aged, highly educated (70% college graduates), employed (78%), White (76%), and slightly more than half were female (57%). Participants drank fairly heavily at baseline, consuming an average of 31 drinks per week. Almost all (91%) participants met diagnostic criteria for moderate-severe alcohol use disorder. There were no differences in participant demographics, baseline clinical characteristics, and drinking severity across treatment groups.
WHAT DID THIS STUDY FIND?
MI and spirit-only MI treatments differed from each other on relational and technical components.
Both MI and spirit-only MI were high on empathy, autonomy support, and collaboration. Spirit-only MI had higher ratings of empathy than full MI. As expected, full MI had higher ratings of evocation, direction, commitment frequency and strength, and structured activities, than spirit-only MI, including evoking more “change talk” than spirit-only MI.
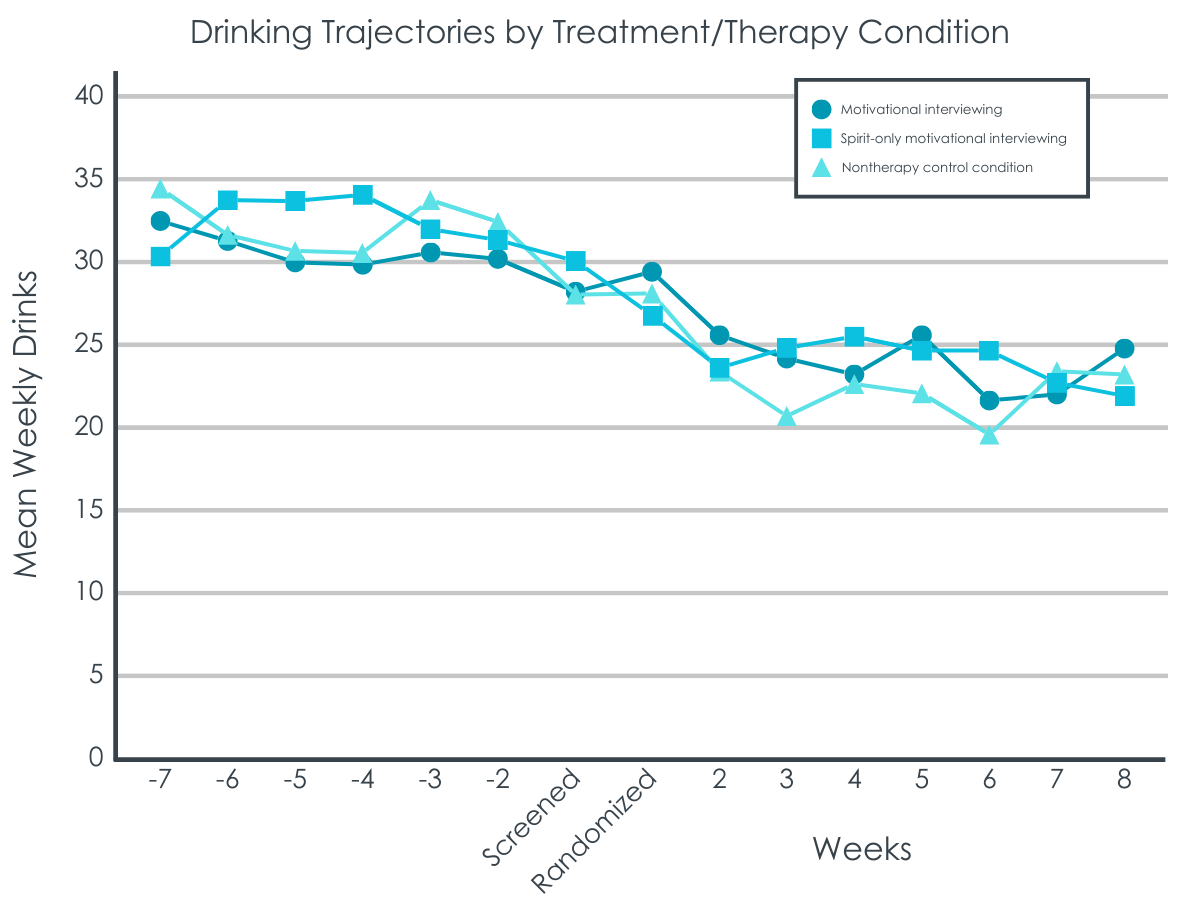
Participants in all three conditions reduced their drinking at the same rate.
Participants did not change their drinking during the first week when answering twice daily surveys before receiving any treatment. Then after receiving treatment, on average, participants reduced their drinking from about 30 drinks per week at screening to 25 drinks per week after 8 weeks. When taking into account participants’ levels of drinking before joining the study, there were no differences in treatment effect between the no therapy condition and full MI or spirit-only MI.
Higher commitment to reduce heavy drinking in the first week predicted greater reductions in drinking regardless of condition.
When taking into account the effect of treatment, for every unit increase in commitment there was a 4% decrease in alcohol use. No treatment was more or less effective for different levels of motivation to reduce drinking.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of adults seeking to reduce heavy drinking who received either full motivational interviewing (MI) intervention, a relational motivational interviewing without directive elements (sprit-only MI), or a brief advice and encouragement to cut down only intervention (no therapy control), there were no differences in reductions in alcohol use by treatment type. All participants cut down by about 5 drinks per week on average over the 8-week study period, regardless of the type of treatment they received. These findings replicate an earlier study by the same researchers that showed no differences across MI, spirit-only MI, and no therapy control in drinking outcomes. In the current study, the only predictor of changes in drinking were participants’ commitment to reduce drinking before receiving any advice or starting treatment.
All participants reduced drinking after being assigned to a treatment, and participants who received brief advice and encouragement to change on their own had equivalent drinking outcomes to those receiving full MI or an MI-informed version of nondirective counseling.
Dismantling randomized clinical trials like the study described here are one of the strongest known methods to test our theories about mobilizers and mechanisms of behavior change, or in other words, why, and what makes, a therapy work. These findings are largely consistent with prior empirical reviews that fail to find consistent support for MI’s hypothesized theory of change (i.e., relational and technical components). Despite MI evoking more “change talk” – a presumed key therapeutic mechanisms of MI – than spirit-only MI, this did not result in greater reductions in alcohol use according to the so-called, technical hypothesis, of MI. And neither type of MI resulted in greater alcohol use reductions than the brief advice condition according to the so-called, relational hypothesis, of MI. It is possible that motivational interviewing works as hypothesized, but only for a specific subpopulation of people with alcohol use disorder and only under certain conditions. For example, in one study the researchers found a positive association between MI consistent therapist behaviors, increased “change talk,” and reduced drinking, but only when therapists were experienced and participants had more severe drinking problems.
In theory, because motivational interviewing is intended to help individuals who are ambivalent or not fully committed to change to engage in a collaborative decision-making process and become more motivated, it would follow then that participants with lower motivation to reduce drinking at the start of the study would benefit more from receiving motivational interviewing, compared to simply receiving brief advice and encouragement to cut down on their own. However, there was no such association in this study.
This lack of finding could be explained by a mismatch between client need and what therapy may be offering. Adults voluntarily seeking treatment and expressing a strong commitment to not drink heavily, as was the case for participants in this study, may have already made the decision to substantially reduce their drinking, which could be dampening the potential intervention effects of motivational interviewing. This analysis did not examine changes in motivation over the study period, so we do not know if participating in full motivational interviewing (MI) or spirit-only MI had a differential effect on motivation than the brief advice and no therapy control condition. Additionally, more research is needed to understand whether providing motivational interviewing to individuals already committed to change might be detrimental when compared to receiving other evidence-supported treatments. For example, using data from a large multi-site study from 1990-1997, researchers found that matching treatment and client attributes tended to optimize already good outcomes, while mismatching had a stronger, negative effect on treatment outcomes. However, it is unclear in this study if the researchers controlled for participation in mutual-help or other treatment use outside of the study – participants who were mismatched could have sought support outside the study (e.g. AA or other mutual-help), which could have dampened the study treatment effect on outcomes.
Finally, it is possible that the twice daily survey, interview with a research assistant about past drinking, and feedback on drinking had an effect on their own that resulted in reduced drinking across conditions and may have obscured differences in outcomes between motivational interview (MI), spirit-only MI had these elements not been present. The brief advice no therapy control condition included a number of components that are present in brief alcohol interventions, like fostering a sense of personal responsibility for changing drinking, feedback on how their drinking compares to other adults in the U.S., and enhancing confidence in their ability to make a change. These elements are also part of MI, but have not been highlighted in theories about how MI works. Additionally, participants completed the twice daily survey and completed in person follow-up assessments.
Participants did not change their drinking during the first week when answering twice daily surveys before receiving any treatment. This helps make a strong case that the interventions delivered throughout the study drove the effect on drinking outcomes, and not the twice-daily surveys. However, some researchers have speculated that follow-up assessments could enhance the efficacy of brief interventions, and is similar to concept in evidence-based psychotherapy practice called “measurement-based care,” in which patient-reported outcome measures are used to track progress in care as part of the therapy process. And while daily surveys have not been found to cause reductions in drinking alone, they may have stronger effects on drinking when combined with a self-change intervention. In summary, it may be that elements of motivational interviewing have their origins in brief interventions, and in combination with aspects of clinical trials research methods, have stronger effects on reducing drinking than anticipated. The current findings suggest further attention and exploration is warranted of whether non-therapy components of MI work to reduce drinking, and if so, how they do it.
This analysis examined baseline levels of motivation to change but did not examine changes in motivation over the study period, which would be useful to see if any of the interventions produced more changes in motivation, or if just the daily survey assessing commitment to reduce drinking created an effect of commitment. The researchers noted that future papers reporting these analyses are forthcoming.
As mentioned by the researchers, participants were randomly assigned to treatment condition and were not assessed for “match” to a particular treatment condition. Additionally, there was no mention of asking participants what they liked or didn’t like about the intervention, or if they thought the intervention was helpful. Client to treatment match may be an underappreciated factor in individualizing alcohol use disorder treatment, so it would be useful to know participants perceptions about the treatment, its effectiveness, and fit for their needs.
One of the strengths of the study is the coding and rating of MI treatment sessions to ensure fidelity and discriminability across conditions (MI and spirit-only MI). However, the researchers did not mention whether raters were blind to therapy condition when coding and making their global ratings. If the raters were not blind to type of MI session, this could introduce significant bias in the coding of the MI treatment sessions.
As mentioned by the researchers, the daily survey could have had a therapeutic effect on drinking (“assessment reactivity”), as it is quite similar to self-monitoring, a skill often used to help make healthy behavior changes. In addition to asking about participants drinking, the survey also asked them to rate their commitment to reduce heavy drinking, which could also have a therapeutic effect. The researchers started the daily survey one week early to measure potential reactivity of the daily survey and found no changes in drinking over one week, however when combined with the feedback received during the baseline assessment, and three additional weeks of daily surveys over the 8 week study period, it is possible this combination and additional time could have affected participants drinking behavior.
Finally, participants in this study were fairly homogenous, meaning results may not be generalizable to more diverse samples. All participants met criteria for mild-moderate alcohol use disorder, were highly educated, mostly White, had to be seeking to cut down but not abstain from drinking at baseline visit. Additionally, they could have no other complicating clinical or social factors including: no other drug use disorder nor frequent (i.e., weekly) drug use; no other social instability (e.g., unstable housing); no risk of self-harm, violence, nor severe psychiatric comorbidities. Although participants were not diverse, this study was well-designed and controlled, as the researchers had a large enough sample to test their question, participant characteristics across the treatment conditions were balanced, the researchers used a rigorous system to ensure the treatment conditions adhered to the intended treatment and were appropriately different from one another, participants had high attendance to treatment sessions and high completion rates of follow-up assessments.
BOTTOM LINE
There are several empirically-supported psychosocial therapies for alcohol use disorder, though key questions remain regarding what treatment elements are driving benefits, for whom do they work best, as well as the optimal time, frequency, and intensity of treatment delivery. Answers to these questions can help refine treatments so that individuals obtain maximum benefits with the most efficient use of time and resources. In this study of 139 adults with alcohol use disorder seeking to reduce (but not abstain from) drinking, who all filled out twice daily surveys and completed 4 in person assessment visits, 4 sessions of full motivational interviewing did no better than one session of brief advice and encouragement to cut down at reducing drinking. This counter-intuitive finding replicates results from an earlier study by the same researchers. The strongest predictor of reducing drinking was motivation to cut down, regardless of any treatment.
For individuals and families seeking recovery: Motivational interviewing (MI) is a widely used counseling approach to resolve ambivalence and enhance motivation to change drinking. This study showed that for adults with problem drinking who are seeking to cut down, receiving brief advice and encouragement to cut down on their own was just as effective as 4 sessions of MI at reducing drinking. Adults seeking to reduce drinking may choose from a range of potentially equally effective, evidence-supported programs depending on needs and preferences. Learn more of different pathways to recovery here.
For treatment professionals and treatment systems: Motivational interviewing (MI) is a widely used counseling approach to resolve ambivalence and enhance motivation to change drinking. This study showed that for adults with problem drinking who are seeking to cut down, receiving brief advice and encouragement to cut down on their own was just as effective as 4 sessions of MI at reducing drinking. A range of evidence-supported programs and interventions may be equally effective for adults with alcohol use disorder seeking to cut down. Providers can ask clients their preferences and tailor recommendations based on client needs. Learn more of different pathways to recovery here.
For scientists:This rigorous dismantling study randomized clinical trial examined 139 adults with alcohol use disorder seeking to reduce (but not abstain from) alcohol use. All participants completed 4 weeks of twice daily EMA over the 8 week study period and in person assessments as screening, randomization, week 5 and week 8. After completing 1 week of EMA, participants received feedback on their drinking and were randomized to receive: 4 sessions of MI, 4 sessions of relational MI without directive elements, or one session of brief advice (normative feedback) and encouragement to cut down with no additional therapy. Of note, there were no differences in changes in drinking by treatment condition. The only predictor of changes in drinking were participants’ commitment to reduce heavy drinking as measured by the first week of EMA before baseline assessment and randomization. Changes in commitment/motivation were not included in this analysis. Future studies should examine client and treatment match, changes in motivation by treatment type, as well as potential therapeutic effects of daily surveys and the timeline follow-back interview when combined with a brief alcohol intervention.
For policy makers: Motivational interviewing (MI) is a widely used counseling approach to resolve ambivalence and enhance motivation to change drinking. This study showed that for adults with problem drinking who are seeking to cut down, receiving brief advice and encouragement to cut down on their own was just as effective as 4 sessions of MI at reducing drinking. A range of evidence-supported programs and interventions may be equally effective for adults with alcohol use disorder seeking to cut down, depending on client characteristics, preferences, and needs. A range of treatment options should be made available for clients to choose from. Learn more of different pathways to recovery here.
Motivational Interviewing (MI), sometimes packaged in a manualized treatment called Motivational Enhancement Therapy (MET), is a widely used counseling approach to resolve ambivalence and enhance motivation to change a behavior. It is most commonly known for its use in alcohol and other drug use treatment and has been used in other health contexts such as smoking cessation, diet and exercise, and HIV risk reduction. Compared to no intervention, or a non-therapy-based intervention (e.g., assessment only or waitlist control), MI has strong empirical support, though it does not do any better than other kinds of interventions.
MI is often delivered as a brief intervention based on client-centered principles, including autonomy and self-determination, support, and positive regard, and emphasizes common counseling skills such as reflective listening, accurate empathy, expressing acceptance of the patient’s goals, and affirmation of the patient’s freedom of choice.
These client-centered principles are sometimes referred to as the “spirit of MI” or the “relational” components of MI. This approach, however, also employs strategies such as selective reinforcement of talk focused on behavior change (“change talk”) and helping the patient realize discrepancies between their values or goals and their actual behavior. These more “directional” strategies are sometimes referred to as the “technical” components of MI. Both “relational” and “technical” components of MI are thought to be necessary to affect behavior change, however research thus far has limited support for either theory. For example, in a meta-analysis of studies that examined the “relational” and “technical” components of MI, the more therapists’ counseling skills were consistent with MI relational and technical components, the more a patient verbalized “change talk” in the counseling session(s). However, the amount patients verbalized “change talk” in the counseling session(s) did not predict their changes in drinking, thus not supporting the presumed theoretical mechanism of how the therapy works.
To try to elucidate what in MI is actually making the difference, this study employed a “dismantling” randomized clinical trial design to pinpoint empirical support for the relational or technical components of MI, by comparing three therapy conditions: Full MI vs spirit-only MI vs non-therapy brief advice. The researchers of this study had conducted a similar study prior that showed no benefit of MI over the non-therapy brief advice. This study addresses limitations of that prior study, including the smaller sample sizes in the prior study, and tests if results could be replicated and are robust. Furthermore, because MI is meant to enhance motivation, the researchers wanted to know if MI would be more helpful for participants who started with lower motivation to reduce drinking than if they had received brief advice and no therapy.
HOW WAS THIS STUDY CONDUCTED?
This randomized clinical trial used a dismantling study design to examine the effects of Motivational Interviewing (MI) on drinking outcomes over 8 weeks among 139 adults seeking help to reduce (but not necessarily abstain from) drinking. Adults seeking to reduce drinking were randomly assigned to receive either:
1 session of brief advice + 4 sessions of motivational interviewing (MI) with all of the standard MI components/features included, called “MI”
1 session of brief advice + 4 sessions of motivational interviewing (MI) with only the relational components/features (without the technical components), called “spirit-only MI”
1 session of brief advice + encouragement to cut down on their own + no therapy
All participants were asked to respond to a twice-daily online survey that included daily reports on their drinking over the 8-week study period.
Participants were recruited via advertisements online and in local media emphasizing a primary goal of reduced drinking (i.e., not abstinence). Interested adults were initially assessed for eligibility using valid and commonly used screeners for alcohol and other drug use, other psychiatric disorders, and cognitive functioning. Participants were included in the study if they were (a) between the ages of 18 and 75, (b) in the past 2 months, drank an average of 15+ drinks per week for women or 24+ drinks per week for men, and (c) met criteria for an Alcohol Use Disorder. Adults were not eligible to participate if they (a) met criteria for another substance use disorder (other than alcohol, cannabis, or nicotine) or used other drugs 2+ times weekly, (b) presented with a serious psychiatric disorder or suicide or violence risk at time of eligibility assessment, (c) had a history of serious alcohol withdrawal symptoms, such as seizures, (d) were legally mandated to substance use treatment, (e) reported social instability (e.g., unstable housing), (f) expressed a desire at eligibility screening to achieve abstinence, or (g) expressed a desire or intent to obtain additional substance use treatment during the 8-week treatment period.
After confirming eligibility, participants were texted twice a day to respond to an online survey asking, “Did you drink yesterday since your morning survey?” When participants responded “yes” to this question, they were asked to report the number of standard drinks of beer, wine, and liquor that they had consumed in the last 24 hours. Participants were also asked about their level of motivation to cut down: “How committed are you to not drink heavily (that is, drink 4 or more drinks for women, 5 or more drinks for men) in the next 24 hours?” Response options ranged from 0 (not at all) to 8 (extremely). Participants received these prompts for the first 2 weeks of the study (i.e., for 1 week after eligibility screening but prior to baseline assessment and randomization to treatment and 1 week following baseline assessment/randomization), as well as during weeks 4 and 7 for a total of 28 days of surveys during the study period.
This daily survey method (called Ecological Momentary Assessment or “EMA”) is meant to get real time, “in the moment” information or with minimal time between the survey and the event, which may be more accurate than asking participants to recall their drinking over a longer period (e.g., past month or more). This frequent assessment may also serve as a form of self-monitoring. Self-monitoring is a commonly used technique when trying to make improvements to a health behavior, such as tracking your steps or keeping a food journal. Bringing greater awareness to a particular behavior alone may change or improve that behavior. Because of this potential therapeutic effect, the researchers started the twice-daily messages 1 week early to test if the twice-daily surveys would influence participants drinking on its own.
After 1 week of twice-daily surveys, participants returned to complete baseline assessment and randomized to receive one of three treatments. During the baseline assessment, participants answered questions about their level of motivation to cut down their drinking (sometimes referred to as “stages of change”) using a psychometrically valid 12-item questionnaire, and completed an interview with a research assistant to record their drinking from the past 8 weeks.
All participants received feedback (brief advice) from a research assistant on their estimated average drinks per week and risk level based on commonly used alcohol use disorder screening measures (low risk, excess of low risk, harmful/hazardous risk, or may be physically dependent) during the baseline assessment. Then participants were randomized to intervention condition. MI and spirit-only MI were both delivered in four sessions that lasted between 45-60 minutes at weeks 1, 2, 5, and 8. Participants randomized to the “no therapy” condition were encouraged to cut down on their own and received no additional treatment.
Recordings of MI and spirit-only MI sessions were reviewed to ensure the study counselors adhered to the specific components of MI intended for the different treatments. Because the study compares different components of MI, it was important for the researchers to ensure that MI and the spirit-only MI were closely following those specific counseling skills and techniques, and that the types of counseling were different from each other. To show this, MI and spirit-only MI sessions were coded with a commonly used MI-specific coding scheme that identifies the specific relational and technical counseling techniques.
In terms of drinking outcomes, first, the analysis tested if there were reductions in drinking over the 8-week study period, and if the treatments were associated with different reductions in alcohol use, controlling for baseline level of use and relevant demographic and clinical characteristics (age, gender, educational and occupational information, race and ethnicity, medical history, family psychiatric and substance abuse history, and the participant’s substance use treatment history). Second, the analysis tested if motivation to change alcohol use was associated with actual reductions in use, and if specific treatments worked better for reducing alcohol use depending on level of motivation. Since MI is meant to enhance motivation, the researchers predicted that the full MI might be more helpful in reducing drinking for participants with low motivation, than participants with higher motivation or other treatment types. The researchers examined both motivation to change at baseline, as well as motivation over time throughout the study from the twice-daily survey.
Participants were mostly middle-aged, highly educated (70% college graduates), employed (78%), White (76%), and slightly more than half were female (57%). Participants drank fairly heavily at baseline, consuming an average of 31 drinks per week. Almost all (91%) participants met diagnostic criteria for moderate-severe alcohol use disorder. There were no differences in participant demographics, baseline clinical characteristics, and drinking severity across treatment groups.
WHAT DID THIS STUDY FIND?
MI and spirit-only MI treatments differed from each other on relational and technical components.
Both MI and spirit-only MI were high on empathy, autonomy support, and collaboration. Spirit-only MI had higher ratings of empathy than full MI. As expected, full MI had higher ratings of evocation, direction, commitment frequency and strength, and structured activities, than spirit-only MI, including evoking more “change talk” than spirit-only MI.
Participants in all three conditions reduced their drinking at the same rate.
Participants did not change their drinking during the first week when answering twice daily surveys before receiving any treatment. Then after receiving treatment, on average, participants reduced their drinking from about 30 drinks per week at screening to 25 drinks per week after 8 weeks. When taking into account participants’ levels of drinking before joining the study, there were no differences in treatment effect between the no therapy condition and full MI or spirit-only MI.
Higher commitment to reduce heavy drinking in the first week predicted greater reductions in drinking regardless of condition.
When taking into account the effect of treatment, for every unit increase in commitment there was a 4% decrease in alcohol use. No treatment was more or less effective for different levels of motivation to reduce drinking.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of adults seeking to reduce heavy drinking who received either full motivational interviewing (MI) intervention, a relational motivational interviewing without directive elements (sprit-only MI), or a brief advice and encouragement to cut down only intervention (no therapy control), there were no differences in reductions in alcohol use by treatment type. All participants cut down by about 5 drinks per week on average over the 8-week study period, regardless of the type of treatment they received. These findings replicate an earlier study by the same researchers that showed no differences across MI, spirit-only MI, and no therapy control in drinking outcomes. In the current study, the only predictor of changes in drinking were participants’ commitment to reduce drinking before receiving any advice or starting treatment.
All participants reduced drinking after being assigned to a treatment, and participants who received brief advice and encouragement to change on their own had equivalent drinking outcomes to those receiving full MI or an MI-informed version of nondirective counseling.
Dismantling randomized clinical trials like the study described here are one of the strongest known methods to test our theories about mobilizers and mechanisms of behavior change, or in other words, why, and what makes, a therapy work. These findings are largely consistent with prior empirical reviews that fail to find consistent support for MI’s hypothesized theory of change (i.e., relational and technical components). Despite MI evoking more “change talk” – a presumed key therapeutic mechanisms of MI – than spirit-only MI, this did not result in greater reductions in alcohol use according to the so-called, technical hypothesis, of MI. And neither type of MI resulted in greater alcohol use reductions than the brief advice condition according to the so-called, relational hypothesis, of MI. It is possible that motivational interviewing works as hypothesized, but only for a specific subpopulation of people with alcohol use disorder and only under certain conditions. For example, in one study the researchers found a positive association between MI consistent therapist behaviors, increased “change talk,” and reduced drinking, but only when therapists were experienced and participants had more severe drinking problems.
In theory, because motivational interviewing is intended to help individuals who are ambivalent or not fully committed to change to engage in a collaborative decision-making process and become more motivated, it would follow then that participants with lower motivation to reduce drinking at the start of the study would benefit more from receiving motivational interviewing, compared to simply receiving brief advice and encouragement to cut down on their own. However, there was no such association in this study.
This lack of finding could be explained by a mismatch between client need and what therapy may be offering. Adults voluntarily seeking treatment and expressing a strong commitment to not drink heavily, as was the case for participants in this study, may have already made the decision to substantially reduce their drinking, which could be dampening the potential intervention effects of motivational interviewing. This analysis did not examine changes in motivation over the study period, so we do not know if participating in full motivational interviewing (MI) or spirit-only MI had a differential effect on motivation than the brief advice and no therapy control condition. Additionally, more research is needed to understand whether providing motivational interviewing to individuals already committed to change might be detrimental when compared to receiving other evidence-supported treatments. For example, using data from a large multi-site study from 1990-1997, researchers found that matching treatment and client attributes tended to optimize already good outcomes, while mismatching had a stronger, negative effect on treatment outcomes. However, it is unclear in this study if the researchers controlled for participation in mutual-help or other treatment use outside of the study – participants who were mismatched could have sought support outside the study (e.g. AA or other mutual-help), which could have dampened the study treatment effect on outcomes.
Finally, it is possible that the twice daily survey, interview with a research assistant about past drinking, and feedback on drinking had an effect on their own that resulted in reduced drinking across conditions and may have obscured differences in outcomes between motivational interview (MI), spirit-only MI had these elements not been present. The brief advice no therapy control condition included a number of components that are present in brief alcohol interventions, like fostering a sense of personal responsibility for changing drinking, feedback on how their drinking compares to other adults in the U.S., and enhancing confidence in their ability to make a change. These elements are also part of MI, but have not been highlighted in theories about how MI works. Additionally, participants completed the twice daily survey and completed in person follow-up assessments.
Participants did not change their drinking during the first week when answering twice daily surveys before receiving any treatment. This helps make a strong case that the interventions delivered throughout the study drove the effect on drinking outcomes, and not the twice-daily surveys. However, some researchers have speculated that follow-up assessments could enhance the efficacy of brief interventions, and is similar to concept in evidence-based psychotherapy practice called “measurement-based care,” in which patient-reported outcome measures are used to track progress in care as part of the therapy process. And while daily surveys have not been found to cause reductions in drinking alone, they may have stronger effects on drinking when combined with a self-change intervention. In summary, it may be that elements of motivational interviewing have their origins in brief interventions, and in combination with aspects of clinical trials research methods, have stronger effects on reducing drinking than anticipated. The current findings suggest further attention and exploration is warranted of whether non-therapy components of MI work to reduce drinking, and if so, how they do it.
This analysis examined baseline levels of motivation to change but did not examine changes in motivation over the study period, which would be useful to see if any of the interventions produced more changes in motivation, or if just the daily survey assessing commitment to reduce drinking created an effect of commitment. The researchers noted that future papers reporting these analyses are forthcoming.
As mentioned by the researchers, participants were randomly assigned to treatment condition and were not assessed for “match” to a particular treatment condition. Additionally, there was no mention of asking participants what they liked or didn’t like about the intervention, or if they thought the intervention was helpful. Client to treatment match may be an underappreciated factor in individualizing alcohol use disorder treatment, so it would be useful to know participants perceptions about the treatment, its effectiveness, and fit for their needs.
One of the strengths of the study is the coding and rating of MI treatment sessions to ensure fidelity and discriminability across conditions (MI and spirit-only MI). However, the researchers did not mention whether raters were blind to therapy condition when coding and making their global ratings. If the raters were not blind to type of MI session, this could introduce significant bias in the coding of the MI treatment sessions.
As mentioned by the researchers, the daily survey could have had a therapeutic effect on drinking (“assessment reactivity”), as it is quite similar to self-monitoring, a skill often used to help make healthy behavior changes. In addition to asking about participants drinking, the survey also asked them to rate their commitment to reduce heavy drinking, which could also have a therapeutic effect. The researchers started the daily survey one week early to measure potential reactivity of the daily survey and found no changes in drinking over one week, however when combined with the feedback received during the baseline assessment, and three additional weeks of daily surveys over the 8 week study period, it is possible this combination and additional time could have affected participants drinking behavior.
Finally, participants in this study were fairly homogenous, meaning results may not be generalizable to more diverse samples. All participants met criteria for mild-moderate alcohol use disorder, were highly educated, mostly White, had to be seeking to cut down but not abstain from drinking at baseline visit. Additionally, they could have no other complicating clinical or social factors including: no other drug use disorder nor frequent (i.e., weekly) drug use; no other social instability (e.g., unstable housing); no risk of self-harm, violence, nor severe psychiatric comorbidities. Although participants were not diverse, this study was well-designed and controlled, as the researchers had a large enough sample to test their question, participant characteristics across the treatment conditions were balanced, the researchers used a rigorous system to ensure the treatment conditions adhered to the intended treatment and were appropriately different from one another, participants had high attendance to treatment sessions and high completion rates of follow-up assessments.
BOTTOM LINE
There are several empirically-supported psychosocial therapies for alcohol use disorder, though key questions remain regarding what treatment elements are driving benefits, for whom do they work best, as well as the optimal time, frequency, and intensity of treatment delivery. Answers to these questions can help refine treatments so that individuals obtain maximum benefits with the most efficient use of time and resources. In this study of 139 adults with alcohol use disorder seeking to reduce (but not abstain from) drinking, who all filled out twice daily surveys and completed 4 in person assessment visits, 4 sessions of full motivational interviewing did no better than one session of brief advice and encouragement to cut down at reducing drinking. This counter-intuitive finding replicates results from an earlier study by the same researchers. The strongest predictor of reducing drinking was motivation to cut down, regardless of any treatment.
For individuals and families seeking recovery: Motivational interviewing (MI) is a widely used counseling approach to resolve ambivalence and enhance motivation to change drinking. This study showed that for adults with problem drinking who are seeking to cut down, receiving brief advice and encouragement to cut down on their own was just as effective as 4 sessions of MI at reducing drinking. Adults seeking to reduce drinking may choose from a range of potentially equally effective, evidence-supported programs depending on needs and preferences. Learn more of different pathways to recovery here.
For treatment professionals and treatment systems: Motivational interviewing (MI) is a widely used counseling approach to resolve ambivalence and enhance motivation to change drinking. This study showed that for adults with problem drinking who are seeking to cut down, receiving brief advice and encouragement to cut down on their own was just as effective as 4 sessions of MI at reducing drinking. A range of evidence-supported programs and interventions may be equally effective for adults with alcohol use disorder seeking to cut down. Providers can ask clients their preferences and tailor recommendations based on client needs. Learn more of different pathways to recovery here.
For scientists:This rigorous dismantling study randomized clinical trial examined 139 adults with alcohol use disorder seeking to reduce (but not abstain from) alcohol use. All participants completed 4 weeks of twice daily EMA over the 8 week study period and in person assessments as screening, randomization, week 5 and week 8. After completing 1 week of EMA, participants received feedback on their drinking and were randomized to receive: 4 sessions of MI, 4 sessions of relational MI without directive elements, or one session of brief advice (normative feedback) and encouragement to cut down with no additional therapy. Of note, there were no differences in changes in drinking by treatment condition. The only predictor of changes in drinking were participants’ commitment to reduce heavy drinking as measured by the first week of EMA before baseline assessment and randomization. Changes in commitment/motivation were not included in this analysis. Future studies should examine client and treatment match, changes in motivation by treatment type, as well as potential therapeutic effects of daily surveys and the timeline follow-back interview when combined with a brief alcohol intervention.
For policy makers: Motivational interviewing (MI) is a widely used counseling approach to resolve ambivalence and enhance motivation to change drinking. This study showed that for adults with problem drinking who are seeking to cut down, receiving brief advice and encouragement to cut down on their own was just as effective as 4 sessions of MI at reducing drinking. A range of evidence-supported programs and interventions may be equally effective for adults with alcohol use disorder seeking to cut down, depending on client characteristics, preferences, and needs. A range of treatment options should be made available for clients to choose from. Learn more of different pathways to recovery here.
Motivational Interviewing (MI), sometimes packaged in a manualized treatment called Motivational Enhancement Therapy (MET), is a widely used counseling approach to resolve ambivalence and enhance motivation to change a behavior. It is most commonly known for its use in alcohol and other drug use treatment and has been used in other health contexts such as smoking cessation, diet and exercise, and HIV risk reduction. Compared to no intervention, or a non-therapy-based intervention (e.g., assessment only or waitlist control), MI has strong empirical support, though it does not do any better than other kinds of interventions.
MI is often delivered as a brief intervention based on client-centered principles, including autonomy and self-determination, support, and positive regard, and emphasizes common counseling skills such as reflective listening, accurate empathy, expressing acceptance of the patient’s goals, and affirmation of the patient’s freedom of choice.
These client-centered principles are sometimes referred to as the “spirit of MI” or the “relational” components of MI. This approach, however, also employs strategies such as selective reinforcement of talk focused on behavior change (“change talk”) and helping the patient realize discrepancies between their values or goals and their actual behavior. These more “directional” strategies are sometimes referred to as the “technical” components of MI. Both “relational” and “technical” components of MI are thought to be necessary to affect behavior change, however research thus far has limited support for either theory. For example, in a meta-analysis of studies that examined the “relational” and “technical” components of MI, the more therapists’ counseling skills were consistent with MI relational and technical components, the more a patient verbalized “change talk” in the counseling session(s). However, the amount patients verbalized “change talk” in the counseling session(s) did not predict their changes in drinking, thus not supporting the presumed theoretical mechanism of how the therapy works.
To try to elucidate what in MI is actually making the difference, this study employed a “dismantling” randomized clinical trial design to pinpoint empirical support for the relational or technical components of MI, by comparing three therapy conditions: Full MI vs spirit-only MI vs non-therapy brief advice. The researchers of this study had conducted a similar study prior that showed no benefit of MI over the non-therapy brief advice. This study addresses limitations of that prior study, including the smaller sample sizes in the prior study, and tests if results could be replicated and are robust. Furthermore, because MI is meant to enhance motivation, the researchers wanted to know if MI would be more helpful for participants who started with lower motivation to reduce drinking than if they had received brief advice and no therapy.
HOW WAS THIS STUDY CONDUCTED?
This randomized clinical trial used a dismantling study design to examine the effects of Motivational Interviewing (MI) on drinking outcomes over 8 weeks among 139 adults seeking help to reduce (but not necessarily abstain from) drinking. Adults seeking to reduce drinking were randomly assigned to receive either:
1 session of brief advice + 4 sessions of motivational interviewing (MI) with all of the standard MI components/features included, called “MI”
1 session of brief advice + 4 sessions of motivational interviewing (MI) with only the relational components/features (without the technical components), called “spirit-only MI”
1 session of brief advice + encouragement to cut down on their own + no therapy
All participants were asked to respond to a twice-daily online survey that included daily reports on their drinking over the 8-week study period.
Participants were recruited via advertisements online and in local media emphasizing a primary goal of reduced drinking (i.e., not abstinence). Interested adults were initially assessed for eligibility using valid and commonly used screeners for alcohol and other drug use, other psychiatric disorders, and cognitive functioning. Participants were included in the study if they were (a) between the ages of 18 and 75, (b) in the past 2 months, drank an average of 15+ drinks per week for women or 24+ drinks per week for men, and (c) met criteria for an Alcohol Use Disorder. Adults were not eligible to participate if they (a) met criteria for another substance use disorder (other than alcohol, cannabis, or nicotine) or used other drugs 2+ times weekly, (b) presented with a serious psychiatric disorder or suicide or violence risk at time of eligibility assessment, (c) had a history of serious alcohol withdrawal symptoms, such as seizures, (d) were legally mandated to substance use treatment, (e) reported social instability (e.g., unstable housing), (f) expressed a desire at eligibility screening to achieve abstinence, or (g) expressed a desire or intent to obtain additional substance use treatment during the 8-week treatment period.
After confirming eligibility, participants were texted twice a day to respond to an online survey asking, “Did you drink yesterday since your morning survey?” When participants responded “yes” to this question, they were asked to report the number of standard drinks of beer, wine, and liquor that they had consumed in the last 24 hours. Participants were also asked about their level of motivation to cut down: “How committed are you to not drink heavily (that is, drink 4 or more drinks for women, 5 or more drinks for men) in the next 24 hours?” Response options ranged from 0 (not at all) to 8 (extremely). Participants received these prompts for the first 2 weeks of the study (i.e., for 1 week after eligibility screening but prior to baseline assessment and randomization to treatment and 1 week following baseline assessment/randomization), as well as during weeks 4 and 7 for a total of 28 days of surveys during the study period.
This daily survey method (called Ecological Momentary Assessment or “EMA”) is meant to get real time, “in the moment” information or with minimal time between the survey and the event, which may be more accurate than asking participants to recall their drinking over a longer period (e.g., past month or more). This frequent assessment may also serve as a form of self-monitoring. Self-monitoring is a commonly used technique when trying to make improvements to a health behavior, such as tracking your steps or keeping a food journal. Bringing greater awareness to a particular behavior alone may change or improve that behavior. Because of this potential therapeutic effect, the researchers started the twice-daily messages 1 week early to test if the twice-daily surveys would influence participants drinking on its own.
After 1 week of twice-daily surveys, participants returned to complete baseline assessment and randomized to receive one of three treatments. During the baseline assessment, participants answered questions about their level of motivation to cut down their drinking (sometimes referred to as “stages of change”) using a psychometrically valid 12-item questionnaire, and completed an interview with a research assistant to record their drinking from the past 8 weeks.
All participants received feedback (brief advice) from a research assistant on their estimated average drinks per week and risk level based on commonly used alcohol use disorder screening measures (low risk, excess of low risk, harmful/hazardous risk, or may be physically dependent) during the baseline assessment. Then participants were randomized to intervention condition. MI and spirit-only MI were both delivered in four sessions that lasted between 45-60 minutes at weeks 1, 2, 5, and 8. Participants randomized to the “no therapy” condition were encouraged to cut down on their own and received no additional treatment.
Recordings of MI and spirit-only MI sessions were reviewed to ensure the study counselors adhered to the specific components of MI intended for the different treatments. Because the study compares different components of MI, it was important for the researchers to ensure that MI and the spirit-only MI were closely following those specific counseling skills and techniques, and that the types of counseling were different from each other. To show this, MI and spirit-only MI sessions were coded with a commonly used MI-specific coding scheme that identifies the specific relational and technical counseling techniques.
In terms of drinking outcomes, first, the analysis tested if there were reductions in drinking over the 8-week study period, and if the treatments were associated with different reductions in alcohol use, controlling for baseline level of use and relevant demographic and clinical characteristics (age, gender, educational and occupational information, race and ethnicity, medical history, family psychiatric and substance abuse history, and the participant’s substance use treatment history). Second, the analysis tested if motivation to change alcohol use was associated with actual reductions in use, and if specific treatments worked better for reducing alcohol use depending on level of motivation. Since MI is meant to enhance motivation, the researchers predicted that the full MI might be more helpful in reducing drinking for participants with low motivation, than participants with higher motivation or other treatment types. The researchers examined both motivation to change at baseline, as well as motivation over time throughout the study from the twice-daily survey.
Participants were mostly middle-aged, highly educated (70% college graduates), employed (78%), White (76%), and slightly more than half were female (57%). Participants drank fairly heavily at baseline, consuming an average of 31 drinks per week. Almost all (91%) participants met diagnostic criteria for moderate-severe alcohol use disorder. There were no differences in participant demographics, baseline clinical characteristics, and drinking severity across treatment groups.
WHAT DID THIS STUDY FIND?
MI and spirit-only MI treatments differed from each other on relational and technical components.
Both MI and spirit-only MI were high on empathy, autonomy support, and collaboration. Spirit-only MI had higher ratings of empathy than full MI. As expected, full MI had higher ratings of evocation, direction, commitment frequency and strength, and structured activities, than spirit-only MI, including evoking more “change talk” than spirit-only MI.
Participants in all three conditions reduced their drinking at the same rate.
Participants did not change their drinking during the first week when answering twice daily surveys before receiving any treatment. Then after receiving treatment, on average, participants reduced their drinking from about 30 drinks per week at screening to 25 drinks per week after 8 weeks. When taking into account participants’ levels of drinking before joining the study, there were no differences in treatment effect between the no therapy condition and full MI or spirit-only MI.
Higher commitment to reduce heavy drinking in the first week predicted greater reductions in drinking regardless of condition.
When taking into account the effect of treatment, for every unit increase in commitment there was a 4% decrease in alcohol use. No treatment was more or less effective for different levels of motivation to reduce drinking.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
In this study of adults seeking to reduce heavy drinking who received either full motivational interviewing (MI) intervention, a relational motivational interviewing without directive elements (sprit-only MI), or a brief advice and encouragement to cut down only intervention (no therapy control), there were no differences in reductions in alcohol use by treatment type. All participants cut down by about 5 drinks per week on average over the 8-week study period, regardless of the type of treatment they received. These findings replicate an earlier study by the same researchers that showed no differences across MI, spirit-only MI, and no therapy control in drinking outcomes. In the current study, the only predictor of changes in drinking were participants’ commitment to reduce drinking before receiving any advice or starting treatment.
All participants reduced drinking after being assigned to a treatment, and participants who received brief advice and encouragement to change on their own had equivalent drinking outcomes to those receiving full MI or an MI-informed version of nondirective counseling.
Dismantling randomized clinical trials like the study described here are one of the strongest known methods to test our theories about mobilizers and mechanisms of behavior change, or in other words, why, and what makes, a therapy work. These findings are largely consistent with prior empirical reviews that fail to find consistent support for MI’s hypothesized theory of change (i.e., relational and technical components). Despite MI evoking more “change talk” – a presumed key therapeutic mechanisms of MI – than spirit-only MI, this did not result in greater reductions in alcohol use according to the so-called, technical hypothesis, of MI. And neither type of MI resulted in greater alcohol use reductions than the brief advice condition according to the so-called, relational hypothesis, of MI. It is possible that motivational interviewing works as hypothesized, but only for a specific subpopulation of people with alcohol use disorder and only under certain conditions. For example, in one study the researchers found a positive association between MI consistent therapist behaviors, increased “change talk,” and reduced drinking, but only when therapists were experienced and participants had more severe drinking problems.
In theory, because motivational interviewing is intended to help individuals who are ambivalent or not fully committed to change to engage in a collaborative decision-making process and become more motivated, it would follow then that participants with lower motivation to reduce drinking at the start of the study would benefit more from receiving motivational interviewing, compared to simply receiving brief advice and encouragement to cut down on their own. However, there was no such association in this study.
This lack of finding could be explained by a mismatch between client need and what therapy may be offering. Adults voluntarily seeking treatment and expressing a strong commitment to not drink heavily, as was the case for participants in this study, may have already made the decision to substantially reduce their drinking, which could be dampening the potential intervention effects of motivational interviewing. This analysis did not examine changes in motivation over the study period, so we do not know if participating in full motivational interviewing (MI) or spirit-only MI had a differential effect on motivation than the brief advice and no therapy control condition. Additionally, more research is needed to understand whether providing motivational interviewing to individuals already committed to change might be detrimental when compared to receiving other evidence-supported treatments. For example, using data from a large multi-site study from 1990-1997, researchers found that matching treatment and client attributes tended to optimize already good outcomes, while mismatching had a stronger, negative effect on treatment outcomes. However, it is unclear in this study if the researchers controlled for participation in mutual-help or other treatment use outside of the study – participants who were mismatched could have sought support outside the study (e.g. AA or other mutual-help), which could have dampened the study treatment effect on outcomes.
Finally, it is possible that the twice daily survey, interview with a research assistant about past drinking, and feedback on drinking had an effect on their own that resulted in reduced drinking across conditions and may have obscured differences in outcomes between motivational interview (MI), spirit-only MI had these elements not been present. The brief advice no therapy control condition included a number of components that are present in brief alcohol interventions, like fostering a sense of personal responsibility for changing drinking, feedback on how their drinking compares to other adults in the U.S., and enhancing confidence in their ability to make a change. These elements are also part of MI, but have not been highlighted in theories about how MI works. Additionally, participants completed the twice daily survey and completed in person follow-up assessments.
Participants did not change their drinking during the first week when answering twice daily surveys before receiving any treatment. This helps make a strong case that the interventions delivered throughout the study drove the effect on drinking outcomes, and not the twice-daily surveys. However, some researchers have speculated that follow-up assessments could enhance the efficacy of brief interventions, and is similar to concept in evidence-based psychotherapy practice called “measurement-based care,” in which patient-reported outcome measures are used to track progress in care as part of the therapy process. And while daily surveys have not been found to cause reductions in drinking alone, they may have stronger effects on drinking when combined with a self-change intervention. In summary, it may be that elements of motivational interviewing have their origins in brief interventions, and in combination with aspects of clinical trials research methods, have stronger effects on reducing drinking than anticipated. The current findings suggest further attention and exploration is warranted of whether non-therapy components of MI work to reduce drinking, and if so, how they do it.
This analysis examined baseline levels of motivation to change but did not examine changes in motivation over the study period, which would be useful to see if any of the interventions produced more changes in motivation, or if just the daily survey assessing commitment to reduce drinking created an effect of commitment. The researchers noted that future papers reporting these analyses are forthcoming.
As mentioned by the researchers, participants were randomly assigned to treatment condition and were not assessed for “match” to a particular treatment condition. Additionally, there was no mention of asking participants what they liked or didn’t like about the intervention, or if they thought the intervention was helpful. Client to treatment match may be an underappreciated factor in individualizing alcohol use disorder treatment, so it would be useful to know participants perceptions about the treatment, its effectiveness, and fit for their needs.
One of the strengths of the study is the coding and rating of MI treatment sessions to ensure fidelity and discriminability across conditions (MI and spirit-only MI). However, the researchers did not mention whether raters were blind to therapy condition when coding and making their global ratings. If the raters were not blind to type of MI session, this could introduce significant bias in the coding of the MI treatment sessions.
As mentioned by the researchers, the daily survey could have had a therapeutic effect on drinking (“assessment reactivity”), as it is quite similar to self-monitoring, a skill often used to help make healthy behavior changes. In addition to asking about participants drinking, the survey also asked them to rate their commitment to reduce heavy drinking, which could also have a therapeutic effect. The researchers started the daily survey one week early to measure potential reactivity of the daily survey and found no changes in drinking over one week, however when combined with the feedback received during the baseline assessment, and three additional weeks of daily surveys over the 8 week study period, it is possible this combination and additional time could have affected participants drinking behavior.
Finally, participants in this study were fairly homogenous, meaning results may not be generalizable to more diverse samples. All participants met criteria for mild-moderate alcohol use disorder, were highly educated, mostly White, had to be seeking to cut down but not abstain from drinking at baseline visit. Additionally, they could have no other complicating clinical or social factors including: no other drug use disorder nor frequent (i.e., weekly) drug use; no other social instability (e.g., unstable housing); no risk of self-harm, violence, nor severe psychiatric comorbidities. Although participants were not diverse, this study was well-designed and controlled, as the researchers had a large enough sample to test their question, participant characteristics across the treatment conditions were balanced, the researchers used a rigorous system to ensure the treatment conditions adhered to the intended treatment and were appropriately different from one another, participants had high attendance to treatment sessions and high completion rates of follow-up assessments.
BOTTOM LINE
There are several empirically-supported psychosocial therapies for alcohol use disorder, though key questions remain regarding what treatment elements are driving benefits, for whom do they work best, as well as the optimal time, frequency, and intensity of treatment delivery. Answers to these questions can help refine treatments so that individuals obtain maximum benefits with the most efficient use of time and resources. In this study of 139 adults with alcohol use disorder seeking to reduce (but not abstain from) drinking, who all filled out twice daily surveys and completed 4 in person assessment visits, 4 sessions of full motivational interviewing did no better than one session of brief advice and encouragement to cut down at reducing drinking. This counter-intuitive finding replicates results from an earlier study by the same researchers. The strongest predictor of reducing drinking was motivation to cut down, regardless of any treatment.
For individuals and families seeking recovery: Motivational interviewing (MI) is a widely used counseling approach to resolve ambivalence and enhance motivation to change drinking. This study showed that for adults with problem drinking who are seeking to cut down, receiving brief advice and encouragement to cut down on their own was just as effective as 4 sessions of MI at reducing drinking. Adults seeking to reduce drinking may choose from a range of potentially equally effective, evidence-supported programs depending on needs and preferences. Learn more of different pathways to recovery here.
For treatment professionals and treatment systems: Motivational interviewing (MI) is a widely used counseling approach to resolve ambivalence and enhance motivation to change drinking. This study showed that for adults with problem drinking who are seeking to cut down, receiving brief advice and encouragement to cut down on their own was just as effective as 4 sessions of MI at reducing drinking. A range of evidence-supported programs and interventions may be equally effective for adults with alcohol use disorder seeking to cut down. Providers can ask clients their preferences and tailor recommendations based on client needs. Learn more of different pathways to recovery here.
For scientists:This rigorous dismantling study randomized clinical trial examined 139 adults with alcohol use disorder seeking to reduce (but not abstain from) alcohol use. All participants completed 4 weeks of twice daily EMA over the 8 week study period and in person assessments as screening, randomization, week 5 and week 8. After completing 1 week of EMA, participants received feedback on their drinking and were randomized to receive: 4 sessions of MI, 4 sessions of relational MI without directive elements, or one session of brief advice (normative feedback) and encouragement to cut down with no additional therapy. Of note, there were no differences in changes in drinking by treatment condition. The only predictor of changes in drinking were participants’ commitment to reduce heavy drinking as measured by the first week of EMA before baseline assessment and randomization. Changes in commitment/motivation were not included in this analysis. Future studies should examine client and treatment match, changes in motivation by treatment type, as well as potential therapeutic effects of daily surveys and the timeline follow-back interview when combined with a brief alcohol intervention.
For policy makers: Motivational interviewing (MI) is a widely used counseling approach to resolve ambivalence and enhance motivation to change drinking. This study showed that for adults with problem drinking who are seeking to cut down, receiving brief advice and encouragement to cut down on their own was just as effective as 4 sessions of MI at reducing drinking. A range of evidence-supported programs and interventions may be equally effective for adults with alcohol use disorder seeking to cut down, depending on client characteristics, preferences, and needs. A range of treatment options should be made available for clients to choose from. Learn more of different pathways to recovery here.