Transgender people have more severe mental health histories and spend more days in substance use disorder treatment than cisgender peers
A lack of research comparing treatment outcomes between cisgender and transgender patients has resulted in a knowledge gap – it is unclear what the specific needs of transgender patients are and how best to address them in treatment. This study analyzed substance use disorder patient care data to determine potential differences in mental health comorbidities and treatment engagement between transgender and cisgender people receiving treatment.
Transgender (i.e., people whose gender identity and/or expression differs from that associated with their sex assigned at birth) are at elevated risk of developing substance use disorders compared to cisgender (a person whose gender identity matches the sex they were assigned at birth) people. There are known differences in mental health comorbidities between cisgender men and women in substance use disorder treatment. For example, research suggests that cisgender women report higher rates of mood and anxiety disorders than cisgender men. Research also suggests that men in substance use treatment are more likely to report personality disorders than women in substance use disorder treatment. These differences are relevant because they may impact an individual’s treatment plan and outcomes. Adapting such interventions for other populations (e.g., transgender people) requires understanding the unique needs of such populations. To date, however, there has been a paucity of research examining the mental health comorbidities of transgender individuals with concurrent substance use disorders. There is a need to better understand the unique needs of the transgender community to better serve their needs in substance use treatment. To this end, the present study compared transgender patients receiving substance use treatment with matched cisgender male and female patients to determine potential differences in mental health comorbidities and treatment engagement.
HOW WAS THIS STUDY CONDUCTED?
The present study was a secondary analysis of self-reported patient survey data. Data were collected at patient intake from a third-party treatment outcome collection provider, Vista Research Group Inc., which contracts with individual facilities to track patient progress during treatment. Through a data use agreement, the Vista Research Group first removed all identifiable information from the data (e.g., patient names) and then transferred it to the authors for analysis.
The primary goal of the present study was to compare comorbidities and treatment engagement between transgender and cisgender patients receiving substance use treatment. Propensity score matching was used to create comparison samples for transgender individuals with cisgender women and cisgender men. Samples were matched using demographic information known to influence substance use and treatment engagement. These included age, education, race and ethnicity, housing (i.e. stable vs. unstable housing), and employment status.
Assessments were delivered to individual patients by their provider via a HIPAA-compliant portal on a computer or tablet. Patients who presented for treatment were asked a series of questions including whether they identified as male, female, or transgender. Patients also completed a series of measures related to their mental health experiences and functioning. Such factors included suicide severity. Patients were also asked about PTSD symptom severity via the PTSD checklist-civilian version. Finally, treatment engagement comparisons were made based on the number of days spent in treatment.
All data were collected from January 2016 – October 2020. The entire sample of patients consisted of 38,091 individuals. Patients came from a variety of treatment facilities including detoxification programs (n = 10,939), partial hospitalization programs (n = 4,752), outpatient SUD programs (n = 3,169), or broad mental health programs (n = 1,835). A total of 64 patients identified themselves as transgender. A sample of demographically matched cisgender men (n = 64) and women (n = 64) were then derived from the entire patient sample. Patients were on average in their late 20s (average ages: transgender = 27.0, cisgender women = 27.4, and cisgender men = 29.3). Most patients identified as non-Hispanic White (70.3%, 60.9%, and 60.9% for transgender, cisgender women and cisgender men respectively). Most participants had stable housing (68.3%, 69.4%, and 63.3% for transgender, cisgender women and cisgender men respectively) and were unemployed (52.4%, 58.1%, and 60.0% for transgender, cisgender women and cisgender men respectively).
WHAT DID THIS STUDY FIND?
Transgender patients reported more suicidal ideation and planning compared to cisgender patients
Transgender patients had higher (more severe) suicide behaviors when entering treatment than both cisgender men and women; these differences were large in magnitude. They were more likely to identify suicide as a reason for entering treatment (40%) compared to cisgender men (11%) and women (14%). They were more likely to have engaged in suicide preparation behavior (39%) than cisgender men (17%); their greater risk than cisgender women (27%) did not reach statistical significance.
Transgender patients reported more PTSD symptoms than cisgender male patients
On average, transgender patients reported a PTSD symptom score of 17.3 whereas cisgender men reported scores of 14.7.
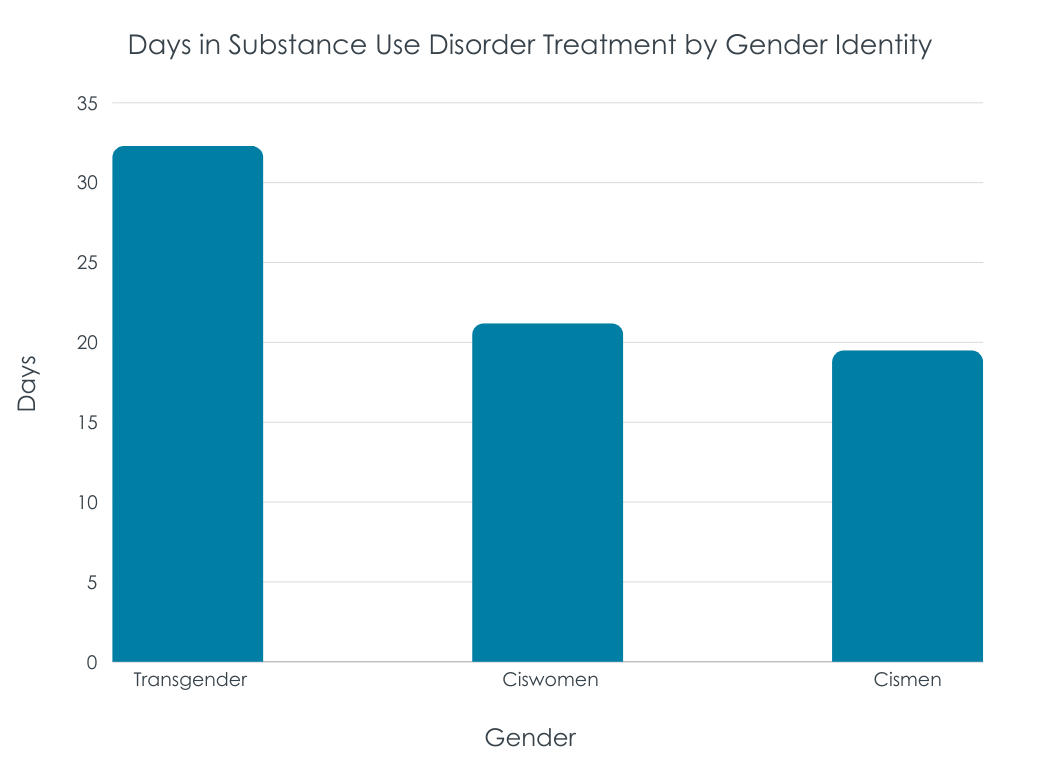
Transgender patients engaged in substance use treatment more than cisgender patients
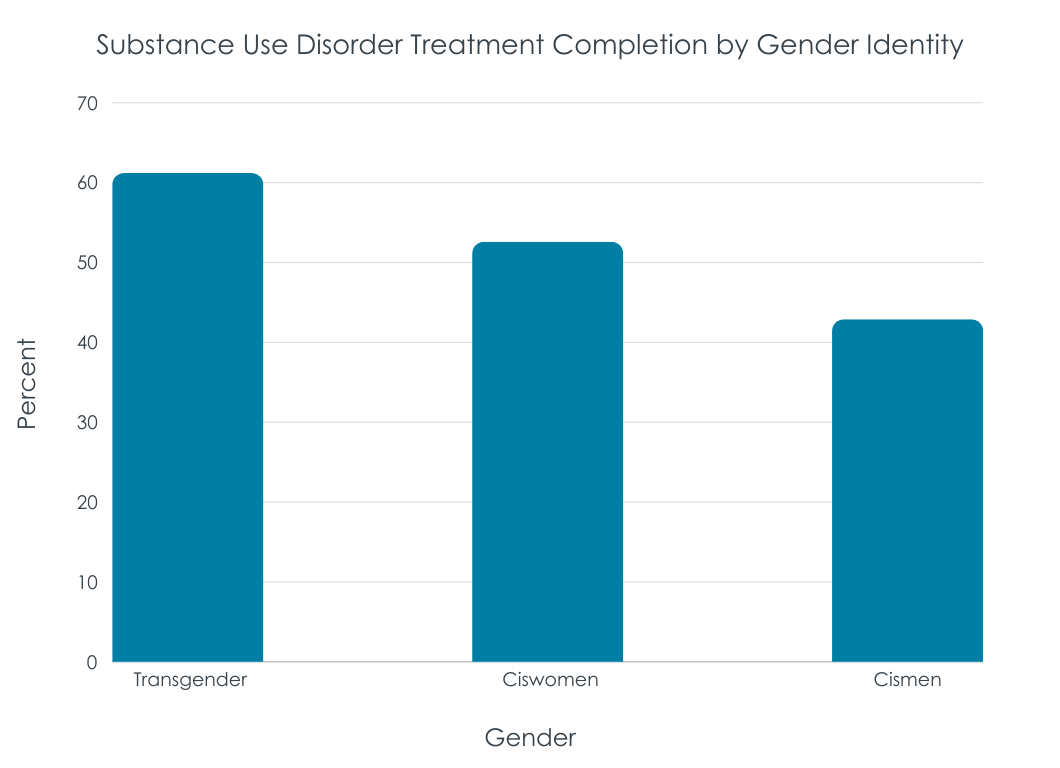
On average transgender patients stayed in substance use treatment for 32.3 days. In contrast, cisgender men and women stayed in treatment for 19.5 and 21.2 days respectively. See figure below. Although the difference between transgender patients and cisgender men was of large magnitude and statistically significant, the medium-sized difference with cisgender women (who had more variability around their average) did not reach statistical significance. Descriptively, transgender patients were more likely to complete treatment (see figure below), but these advantages were not statistically significant.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that transgender substance use treatment patients experience more severe suicidal ideation and PTSD symptoms than cisgender patients. Transgender patients endorsed more suicide scale items than cisgender patients and screened positive for suicide risk more often than cisgender male patients. Furthermore, transgender patients were more likely to report intentions to act upon suicidal thoughts than cisgender female patients. Transgender patients also had higher PTSD symptom scores than cisgender male patients. There was also evidence that transgender patients engaged in treatment longer than cisgender male patients. The use of propensity scores to create matched samples of cisgender males and females to which transgender individuals could be compared was a strength of the study.
Taken together, these results may indicate that transgender people with substance use disorders suffer from more severe and concerning comorbid mental health issues. This greater clinical severity, and potentially greater subjective distress, among transgender individuals may explain why they are in treatment for a longer duration than cisgender individuals. Such mental health challenges – and potential need for longer treatment duration – should be considered when tailoring treatment for individuals from this population. To date, there is a dearth of research examining how efficacious current interventions are at treating substance use disorder among transgender patients. Furthermore, there is a lack of work examining how to tailor substance use disorder care for transgender people. More consulting specifically with transgender individuals with this lived experience could help inform this. The small sample of transgender individuals made it more difficult to detect significant differences between this unique, at-risk, group and their cisgender counterparts. There remains a lot of work to be done on how best to meet the needs of transgender Individuals with substance use disorders.
The current research used a very narrow definition of transgender- people presenting for treatment were asked whether they identified as male, female, or transgender. No other information about gender identity or sex assigned at birth was available. Therefore, only individuals who self-identified as transgender were included in the analyses. For example, individuals presenting for care whose gender identity was incongruent with their sex assigned at birth but did not identify specifically as transgender (e.g., those who identified as male/female but were assigned female/male respectively at birth) were not included in the transgender group. Furthermore, the present study did not include people from other gender minority groups (e.g., gender non-binary individuals). This is a limitation as it severely limits our ability to infer the health needs of the gender minority community broadly. Evidence suggests that health disparities exist between the cisgender and gender minority communities as well as between members of the gender minority community.
The way in which gender identity was collected may have led to an underreporting of transgender identity. As described previously, people presenting for treatment were asked whether they identified as male, female, or transgender. It is possible that some transgender patients felt uncomfortable disclosing their identity due to concerns of being stigmatized. Alternatively, some patients may have identified as male/female but were assigned a different sex at birth (e.g., they had transitioned socially to a different gender identity). The underreporting of transgender patients is supported, in part, by research estimating that transgender/gender diverse adults make up ~.5% of the US population. The current sample of 64 patients is ~.1% of the entire population of patients in care all treatment sites. Had the sample been representative of the US population of gender diverse people we can assume the proportion would have been higher.
Similarly, the current study does not specify where patients were receiving care. For example, although patients received care at a range of facilities including detoxification programs, partial hospitalization programs, and programs treating mental health broadly, it is not specified if there were differences in where treatment was received between transgender and cisgender patients. It is likely that those seeking care from mental health programs (1835 of the 38,091 total patient sample) were more likely to have mental health difficulties than those receiving substance use disorder care specifically.
BOTTOM LINE
This study found that transgender patients receiving substance use disorder care may suffer from more severe and concerning mental health comorbidities compared to cisgender patients. The authors found that transgender patients entered treatment with more suicide risk and past suicide behaviors. Transgender patients also endorsed an intent to act upon their suicidal thoughts more often than cisgender women. The authors also found that transgender patients reported more PTSD symptoms than cisgender male patients. At the same time, transgender patients had longer treatment duration than both cisgender men and women, potentially explained by their greater clinical severity. Also, given the greater stigma against transgender people, it is a positive that they may have felt welcomed and comfortable enough to stay longer in these treatment settings, but these experiences should be examined in more detail. Given the limitations of the data, it is likely that the results are not representative of the general gender minority population. Nevertheless, the present study is an important first step in elucidating the unique care needs of the transgender community. There remains significant substance use related health disparities between cisgender and transgender adults in the US. It is critical for more research to be conducted on the unique needs of the transgender community and how providers and public health officials can better serve them.
For individuals and families seeking recovery: The present study showed that transgender patients receiving substance use disorder treatment had specific and severe mental health comorbidities compared to cisgender patients. This suggests that those seeking recovery services for themselves, or others may need to look for services capable of meeting the unique needs of transgender patients. For example, seeking providers who have experience working with the LGBT community and/or who have received special training in fields relevant for these populations (e.g., gender affirming care). It is important, however, that those seeking providers confirm before initiating care that relevant services are being provided. Although many providers list that they offer LGBT-specific care (e.g., on their website) evidence suggests that over 80% of agencies which indicated they provide services specifically for the LGBT community did not in fact offer such services.
For treatment professionals and treatment systems: The present study suggests that transgender individuals receiving treatment for substance use disorder experience severe suicidal ideation and PTSD symptoms. Therefore, it is important for those working with this population to be trained in screening for, and assessing and treating, mental health issues, notably suicidal histories and current risks. It is also important for providers to be cognizant of potential barriers members of the gender minority community may face in accessing and utilizing care (e.g., social stigma towards transgender people). It may be helpful for providers and clinical staff to assess their current care environment and determine how it may need to be modified to accommodate the needs of the gender minority community. In addition, speaking frankly with gender minority patients about potential knowledge gaps and eliciting from them their unique needs can help build a strong patient-provider relationship and improve care.
For scientists: Scientists would do well to conduct research on the unique needs of transgender patients receiving substance use disorder care. To date, there has been a paucity of work examining how interventions can best be tailored to meet the needs of this population. Furthermore, there are currently significant basic science gaps – for example, it is unknown how gender affirming care (hormone therapy) may moderate the physiological impact of alcohol use on the body, making harm reduction-related recommendations more challenging. In addition, it is unclear how being a member of the LGBT+ community influences physical, mental, and social health long term. The Pride Study, the first large scale longitudinal cohort study of LGBT+ individuals, will hopefully elucidate some of these ambiguities in the future, but in the interim more work is needed in this area.
For policy makers: Policy makers would do well to consider implementing programs to address the mental health needs of patients in substance use treatment who are also members of the transgender community. One solution could be to reduce barriers to mental health and substance use treatment (e.g., through Medicaid). This could include partnering with local LGBT foundations to ensure funding is available for outreach. In addition, the evidence that transgender patients were more likely to report PTSD symptoms suggests that it may be important for policy makers to develop and implement strategies that reduce the harms of trauma on gender minority populations. That is, if experiencing trauma is a risk factor for mental health issues then reducing its impact may be beneficial in reducing said problems. Such efforts could take the form of outreach programs targeting members of the LGBT community.
Transgender (i.e., people whose gender identity and/or expression differs from that associated with their sex assigned at birth) are at elevated risk of developing substance use disorders compared to cisgender (a person whose gender identity matches the sex they were assigned at birth) people. There are known differences in mental health comorbidities between cisgender men and women in substance use disorder treatment. For example, research suggests that cisgender women report higher rates of mood and anxiety disorders than cisgender men. Research also suggests that men in substance use treatment are more likely to report personality disorders than women in substance use disorder treatment. These differences are relevant because they may impact an individual’s treatment plan and outcomes. Adapting such interventions for other populations (e.g., transgender people) requires understanding the unique needs of such populations. To date, however, there has been a paucity of research examining the mental health comorbidities of transgender individuals with concurrent substance use disorders. There is a need to better understand the unique needs of the transgender community to better serve their needs in substance use treatment. To this end, the present study compared transgender patients receiving substance use treatment with matched cisgender male and female patients to determine potential differences in mental health comorbidities and treatment engagement.
HOW WAS THIS STUDY CONDUCTED?
The present study was a secondary analysis of self-reported patient survey data. Data were collected at patient intake from a third-party treatment outcome collection provider, Vista Research Group Inc., which contracts with individual facilities to track patient progress during treatment. Through a data use agreement, the Vista Research Group first removed all identifiable information from the data (e.g., patient names) and then transferred it to the authors for analysis.
The primary goal of the present study was to compare comorbidities and treatment engagement between transgender and cisgender patients receiving substance use treatment. Propensity score matching was used to create comparison samples for transgender individuals with cisgender women and cisgender men. Samples were matched using demographic information known to influence substance use and treatment engagement. These included age, education, race and ethnicity, housing (i.e. stable vs. unstable housing), and employment status.
Assessments were delivered to individual patients by their provider via a HIPAA-compliant portal on a computer or tablet. Patients who presented for treatment were asked a series of questions including whether they identified as male, female, or transgender. Patients also completed a series of measures related to their mental health experiences and functioning. Such factors included suicide severity. Patients were also asked about PTSD symptom severity via the PTSD checklist-civilian version. Finally, treatment engagement comparisons were made based on the number of days spent in treatment.
All data were collected from January 2016 – October 2020. The entire sample of patients consisted of 38,091 individuals. Patients came from a variety of treatment facilities including detoxification programs (n = 10,939), partial hospitalization programs (n = 4,752), outpatient SUD programs (n = 3,169), or broad mental health programs (n = 1,835). A total of 64 patients identified themselves as transgender. A sample of demographically matched cisgender men (n = 64) and women (n = 64) were then derived from the entire patient sample. Patients were on average in their late 20s (average ages: transgender = 27.0, cisgender women = 27.4, and cisgender men = 29.3). Most patients identified as non-Hispanic White (70.3%, 60.9%, and 60.9% for transgender, cisgender women and cisgender men respectively). Most participants had stable housing (68.3%, 69.4%, and 63.3% for transgender, cisgender women and cisgender men respectively) and were unemployed (52.4%, 58.1%, and 60.0% for transgender, cisgender women and cisgender men respectively).
WHAT DID THIS STUDY FIND?
Transgender patients reported more suicidal ideation and planning compared to cisgender patients
Transgender patients had higher (more severe) suicide behaviors when entering treatment than both cisgender men and women; these differences were large in magnitude. They were more likely to identify suicide as a reason for entering treatment (40%) compared to cisgender men (11%) and women (14%). They were more likely to have engaged in suicide preparation behavior (39%) than cisgender men (17%); their greater risk than cisgender women (27%) did not reach statistical significance.
Transgender patients reported more PTSD symptoms than cisgender male patients
On average, transgender patients reported a PTSD symptom score of 17.3 whereas cisgender men reported scores of 14.7.
Transgender patients engaged in substance use treatment more than cisgender patients
On average transgender patients stayed in substance use treatment for 32.3 days. In contrast, cisgender men and women stayed in treatment for 19.5 and 21.2 days respectively. See figure below. Although the difference between transgender patients and cisgender men was of large magnitude and statistically significant, the medium-sized difference with cisgender women (who had more variability around their average) did not reach statistical significance. Descriptively, transgender patients were more likely to complete treatment (see figure below), but these advantages were not statistically significant.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that transgender substance use treatment patients experience more severe suicidal ideation and PTSD symptoms than cisgender patients. Transgender patients endorsed more suicide scale items than cisgender patients and screened positive for suicide risk more often than cisgender male patients. Furthermore, transgender patients were more likely to report intentions to act upon suicidal thoughts than cisgender female patients. Transgender patients also had higher PTSD symptom scores than cisgender male patients. There was also evidence that transgender patients engaged in treatment longer than cisgender male patients. The use of propensity scores to create matched samples of cisgender males and females to which transgender individuals could be compared was a strength of the study.
Taken together, these results may indicate that transgender people with substance use disorders suffer from more severe and concerning comorbid mental health issues. This greater clinical severity, and potentially greater subjective distress, among transgender individuals may explain why they are in treatment for a longer duration than cisgender individuals. Such mental health challenges – and potential need for longer treatment duration – should be considered when tailoring treatment for individuals from this population. To date, there is a dearth of research examining how efficacious current interventions are at treating substance use disorder among transgender patients. Furthermore, there is a lack of work examining how to tailor substance use disorder care for transgender people. More consulting specifically with transgender individuals with this lived experience could help inform this. The small sample of transgender individuals made it more difficult to detect significant differences between this unique, at-risk, group and their cisgender counterparts. There remains a lot of work to be done on how best to meet the needs of transgender Individuals with substance use disorders.
The current research used a very narrow definition of transgender- people presenting for treatment were asked whether they identified as male, female, or transgender. No other information about gender identity or sex assigned at birth was available. Therefore, only individuals who self-identified as transgender were included in the analyses. For example, individuals presenting for care whose gender identity was incongruent with their sex assigned at birth but did not identify specifically as transgender (e.g., those who identified as male/female but were assigned female/male respectively at birth) were not included in the transgender group. Furthermore, the present study did not include people from other gender minority groups (e.g., gender non-binary individuals). This is a limitation as it severely limits our ability to infer the health needs of the gender minority community broadly. Evidence suggests that health disparities exist between the cisgender and gender minority communities as well as between members of the gender minority community.
The way in which gender identity was collected may have led to an underreporting of transgender identity. As described previously, people presenting for treatment were asked whether they identified as male, female, or transgender. It is possible that some transgender patients felt uncomfortable disclosing their identity due to concerns of being stigmatized. Alternatively, some patients may have identified as male/female but were assigned a different sex at birth (e.g., they had transitioned socially to a different gender identity). The underreporting of transgender patients is supported, in part, by research estimating that transgender/gender diverse adults make up ~.5% of the US population. The current sample of 64 patients is ~.1% of the entire population of patients in care all treatment sites. Had the sample been representative of the US population of gender diverse people we can assume the proportion would have been higher.
Similarly, the current study does not specify where patients were receiving care. For example, although patients received care at a range of facilities including detoxification programs, partial hospitalization programs, and programs treating mental health broadly, it is not specified if there were differences in where treatment was received between transgender and cisgender patients. It is likely that those seeking care from mental health programs (1835 of the 38,091 total patient sample) were more likely to have mental health difficulties than those receiving substance use disorder care specifically.
BOTTOM LINE
This study found that transgender patients receiving substance use disorder care may suffer from more severe and concerning mental health comorbidities compared to cisgender patients. The authors found that transgender patients entered treatment with more suicide risk and past suicide behaviors. Transgender patients also endorsed an intent to act upon their suicidal thoughts more often than cisgender women. The authors also found that transgender patients reported more PTSD symptoms than cisgender male patients. At the same time, transgender patients had longer treatment duration than both cisgender men and women, potentially explained by their greater clinical severity. Also, given the greater stigma against transgender people, it is a positive that they may have felt welcomed and comfortable enough to stay longer in these treatment settings, but these experiences should be examined in more detail. Given the limitations of the data, it is likely that the results are not representative of the general gender minority population. Nevertheless, the present study is an important first step in elucidating the unique care needs of the transgender community. There remains significant substance use related health disparities between cisgender and transgender adults in the US. It is critical for more research to be conducted on the unique needs of the transgender community and how providers and public health officials can better serve them.
For individuals and families seeking recovery: The present study showed that transgender patients receiving substance use disorder treatment had specific and severe mental health comorbidities compared to cisgender patients. This suggests that those seeking recovery services for themselves, or others may need to look for services capable of meeting the unique needs of transgender patients. For example, seeking providers who have experience working with the LGBT community and/or who have received special training in fields relevant for these populations (e.g., gender affirming care). It is important, however, that those seeking providers confirm before initiating care that relevant services are being provided. Although many providers list that they offer LGBT-specific care (e.g., on their website) evidence suggests that over 80% of agencies which indicated they provide services specifically for the LGBT community did not in fact offer such services.
For treatment professionals and treatment systems: The present study suggests that transgender individuals receiving treatment for substance use disorder experience severe suicidal ideation and PTSD symptoms. Therefore, it is important for those working with this population to be trained in screening for, and assessing and treating, mental health issues, notably suicidal histories and current risks. It is also important for providers to be cognizant of potential barriers members of the gender minority community may face in accessing and utilizing care (e.g., social stigma towards transgender people). It may be helpful for providers and clinical staff to assess their current care environment and determine how it may need to be modified to accommodate the needs of the gender minority community. In addition, speaking frankly with gender minority patients about potential knowledge gaps and eliciting from them their unique needs can help build a strong patient-provider relationship and improve care.
For scientists: Scientists would do well to conduct research on the unique needs of transgender patients receiving substance use disorder care. To date, there has been a paucity of work examining how interventions can best be tailored to meet the needs of this population. Furthermore, there are currently significant basic science gaps – for example, it is unknown how gender affirming care (hormone therapy) may moderate the physiological impact of alcohol use on the body, making harm reduction-related recommendations more challenging. In addition, it is unclear how being a member of the LGBT+ community influences physical, mental, and social health long term. The Pride Study, the first large scale longitudinal cohort study of LGBT+ individuals, will hopefully elucidate some of these ambiguities in the future, but in the interim more work is needed in this area.
For policy makers: Policy makers would do well to consider implementing programs to address the mental health needs of patients in substance use treatment who are also members of the transgender community. One solution could be to reduce barriers to mental health and substance use treatment (e.g., through Medicaid). This could include partnering with local LGBT foundations to ensure funding is available for outreach. In addition, the evidence that transgender patients were more likely to report PTSD symptoms suggests that it may be important for policy makers to develop and implement strategies that reduce the harms of trauma on gender minority populations. That is, if experiencing trauma is a risk factor for mental health issues then reducing its impact may be beneficial in reducing said problems. Such efforts could take the form of outreach programs targeting members of the LGBT community.
Transgender (i.e., people whose gender identity and/or expression differs from that associated with their sex assigned at birth) are at elevated risk of developing substance use disorders compared to cisgender (a person whose gender identity matches the sex they were assigned at birth) people. There are known differences in mental health comorbidities between cisgender men and women in substance use disorder treatment. For example, research suggests that cisgender women report higher rates of mood and anxiety disorders than cisgender men. Research also suggests that men in substance use treatment are more likely to report personality disorders than women in substance use disorder treatment. These differences are relevant because they may impact an individual’s treatment plan and outcomes. Adapting such interventions for other populations (e.g., transgender people) requires understanding the unique needs of such populations. To date, however, there has been a paucity of research examining the mental health comorbidities of transgender individuals with concurrent substance use disorders. There is a need to better understand the unique needs of the transgender community to better serve their needs in substance use treatment. To this end, the present study compared transgender patients receiving substance use treatment with matched cisgender male and female patients to determine potential differences in mental health comorbidities and treatment engagement.
HOW WAS THIS STUDY CONDUCTED?
The present study was a secondary analysis of self-reported patient survey data. Data were collected at patient intake from a third-party treatment outcome collection provider, Vista Research Group Inc., which contracts with individual facilities to track patient progress during treatment. Through a data use agreement, the Vista Research Group first removed all identifiable information from the data (e.g., patient names) and then transferred it to the authors for analysis.
The primary goal of the present study was to compare comorbidities and treatment engagement between transgender and cisgender patients receiving substance use treatment. Propensity score matching was used to create comparison samples for transgender individuals with cisgender women and cisgender men. Samples were matched using demographic information known to influence substance use and treatment engagement. These included age, education, race and ethnicity, housing (i.e. stable vs. unstable housing), and employment status.
Assessments were delivered to individual patients by their provider via a HIPAA-compliant portal on a computer or tablet. Patients who presented for treatment were asked a series of questions including whether they identified as male, female, or transgender. Patients also completed a series of measures related to their mental health experiences and functioning. Such factors included suicide severity. Patients were also asked about PTSD symptom severity via the PTSD checklist-civilian version. Finally, treatment engagement comparisons were made based on the number of days spent in treatment.
All data were collected from January 2016 – October 2020. The entire sample of patients consisted of 38,091 individuals. Patients came from a variety of treatment facilities including detoxification programs (n = 10,939), partial hospitalization programs (n = 4,752), outpatient SUD programs (n = 3,169), or broad mental health programs (n = 1,835). A total of 64 patients identified themselves as transgender. A sample of demographically matched cisgender men (n = 64) and women (n = 64) were then derived from the entire patient sample. Patients were on average in their late 20s (average ages: transgender = 27.0, cisgender women = 27.4, and cisgender men = 29.3). Most patients identified as non-Hispanic White (70.3%, 60.9%, and 60.9% for transgender, cisgender women and cisgender men respectively). Most participants had stable housing (68.3%, 69.4%, and 63.3% for transgender, cisgender women and cisgender men respectively) and were unemployed (52.4%, 58.1%, and 60.0% for transgender, cisgender women and cisgender men respectively).
WHAT DID THIS STUDY FIND?
Transgender patients reported more suicidal ideation and planning compared to cisgender patients
Transgender patients had higher (more severe) suicide behaviors when entering treatment than both cisgender men and women; these differences were large in magnitude. They were more likely to identify suicide as a reason for entering treatment (40%) compared to cisgender men (11%) and women (14%). They were more likely to have engaged in suicide preparation behavior (39%) than cisgender men (17%); their greater risk than cisgender women (27%) did not reach statistical significance.
Transgender patients reported more PTSD symptoms than cisgender male patients
On average, transgender patients reported a PTSD symptom score of 17.3 whereas cisgender men reported scores of 14.7.
Transgender patients engaged in substance use treatment more than cisgender patients
On average transgender patients stayed in substance use treatment for 32.3 days. In contrast, cisgender men and women stayed in treatment for 19.5 and 21.2 days respectively. See figure below. Although the difference between transgender patients and cisgender men was of large magnitude and statistically significant, the medium-sized difference with cisgender women (who had more variability around their average) did not reach statistical significance. Descriptively, transgender patients were more likely to complete treatment (see figure below), but these advantages were not statistically significant.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that transgender substance use treatment patients experience more severe suicidal ideation and PTSD symptoms than cisgender patients. Transgender patients endorsed more suicide scale items than cisgender patients and screened positive for suicide risk more often than cisgender male patients. Furthermore, transgender patients were more likely to report intentions to act upon suicidal thoughts than cisgender female patients. Transgender patients also had higher PTSD symptom scores than cisgender male patients. There was also evidence that transgender patients engaged in treatment longer than cisgender male patients. The use of propensity scores to create matched samples of cisgender males and females to which transgender individuals could be compared was a strength of the study.
Taken together, these results may indicate that transgender people with substance use disorders suffer from more severe and concerning comorbid mental health issues. This greater clinical severity, and potentially greater subjective distress, among transgender individuals may explain why they are in treatment for a longer duration than cisgender individuals. Such mental health challenges – and potential need for longer treatment duration – should be considered when tailoring treatment for individuals from this population. To date, there is a dearth of research examining how efficacious current interventions are at treating substance use disorder among transgender patients. Furthermore, there is a lack of work examining how to tailor substance use disorder care for transgender people. More consulting specifically with transgender individuals with this lived experience could help inform this. The small sample of transgender individuals made it more difficult to detect significant differences between this unique, at-risk, group and their cisgender counterparts. There remains a lot of work to be done on how best to meet the needs of transgender Individuals with substance use disorders.
The current research used a very narrow definition of transgender- people presenting for treatment were asked whether they identified as male, female, or transgender. No other information about gender identity or sex assigned at birth was available. Therefore, only individuals who self-identified as transgender were included in the analyses. For example, individuals presenting for care whose gender identity was incongruent with their sex assigned at birth but did not identify specifically as transgender (e.g., those who identified as male/female but were assigned female/male respectively at birth) were not included in the transgender group. Furthermore, the present study did not include people from other gender minority groups (e.g., gender non-binary individuals). This is a limitation as it severely limits our ability to infer the health needs of the gender minority community broadly. Evidence suggests that health disparities exist between the cisgender and gender minority communities as well as between members of the gender minority community.
The way in which gender identity was collected may have led to an underreporting of transgender identity. As described previously, people presenting for treatment were asked whether they identified as male, female, or transgender. It is possible that some transgender patients felt uncomfortable disclosing their identity due to concerns of being stigmatized. Alternatively, some patients may have identified as male/female but were assigned a different sex at birth (e.g., they had transitioned socially to a different gender identity). The underreporting of transgender patients is supported, in part, by research estimating that transgender/gender diverse adults make up ~.5% of the US population. The current sample of 64 patients is ~.1% of the entire population of patients in care all treatment sites. Had the sample been representative of the US population of gender diverse people we can assume the proportion would have been higher.
Similarly, the current study does not specify where patients were receiving care. For example, although patients received care at a range of facilities including detoxification programs, partial hospitalization programs, and programs treating mental health broadly, it is not specified if there were differences in where treatment was received between transgender and cisgender patients. It is likely that those seeking care from mental health programs (1835 of the 38,091 total patient sample) were more likely to have mental health difficulties than those receiving substance use disorder care specifically.
BOTTOM LINE
This study found that transgender patients receiving substance use disorder care may suffer from more severe and concerning mental health comorbidities compared to cisgender patients. The authors found that transgender patients entered treatment with more suicide risk and past suicide behaviors. Transgender patients also endorsed an intent to act upon their suicidal thoughts more often than cisgender women. The authors also found that transgender patients reported more PTSD symptoms than cisgender male patients. At the same time, transgender patients had longer treatment duration than both cisgender men and women, potentially explained by their greater clinical severity. Also, given the greater stigma against transgender people, it is a positive that they may have felt welcomed and comfortable enough to stay longer in these treatment settings, but these experiences should be examined in more detail. Given the limitations of the data, it is likely that the results are not representative of the general gender minority population. Nevertheless, the present study is an important first step in elucidating the unique care needs of the transgender community. There remains significant substance use related health disparities between cisgender and transgender adults in the US. It is critical for more research to be conducted on the unique needs of the transgender community and how providers and public health officials can better serve them.
For individuals and families seeking recovery: The present study showed that transgender patients receiving substance use disorder treatment had specific and severe mental health comorbidities compared to cisgender patients. This suggests that those seeking recovery services for themselves, or others may need to look for services capable of meeting the unique needs of transgender patients. For example, seeking providers who have experience working with the LGBT community and/or who have received special training in fields relevant for these populations (e.g., gender affirming care). It is important, however, that those seeking providers confirm before initiating care that relevant services are being provided. Although many providers list that they offer LGBT-specific care (e.g., on their website) evidence suggests that over 80% of agencies which indicated they provide services specifically for the LGBT community did not in fact offer such services.
For treatment professionals and treatment systems: The present study suggests that transgender individuals receiving treatment for substance use disorder experience severe suicidal ideation and PTSD symptoms. Therefore, it is important for those working with this population to be trained in screening for, and assessing and treating, mental health issues, notably suicidal histories and current risks. It is also important for providers to be cognizant of potential barriers members of the gender minority community may face in accessing and utilizing care (e.g., social stigma towards transgender people). It may be helpful for providers and clinical staff to assess their current care environment and determine how it may need to be modified to accommodate the needs of the gender minority community. In addition, speaking frankly with gender minority patients about potential knowledge gaps and eliciting from them their unique needs can help build a strong patient-provider relationship and improve care.
For scientists: Scientists would do well to conduct research on the unique needs of transgender patients receiving substance use disorder care. To date, there has been a paucity of work examining how interventions can best be tailored to meet the needs of this population. Furthermore, there are currently significant basic science gaps – for example, it is unknown how gender affirming care (hormone therapy) may moderate the physiological impact of alcohol use on the body, making harm reduction-related recommendations more challenging. In addition, it is unclear how being a member of the LGBT+ community influences physical, mental, and social health long term. The Pride Study, the first large scale longitudinal cohort study of LGBT+ individuals, will hopefully elucidate some of these ambiguities in the future, but in the interim more work is needed in this area.
For policy makers: Policy makers would do well to consider implementing programs to address the mental health needs of patients in substance use treatment who are also members of the transgender community. One solution could be to reduce barriers to mental health and substance use treatment (e.g., through Medicaid). This could include partnering with local LGBT foundations to ensure funding is available for outreach. In addition, the evidence that transgender patients were more likely to report PTSD symptoms suggests that it may be important for policy makers to develop and implement strategies that reduce the harms of trauma on gender minority populations. That is, if experiencing trauma is a risk factor for mental health issues then reducing its impact may be beneficial in reducing said problems. Such efforts could take the form of outreach programs targeting members of the LGBT community.