“Traveling Companions”: Results of a patient navigation intervention for pregnant people with opioid use disorder
Since 2010, opioid use related diagnoses have increased dramatically among people immediately after giving birth (i.e., postpartum). This study tested a novel “patient navigation” intervention designed to facilitate opioid use disorder care and reduce non-medical opioid use.
It is unclear why relapse rates are so high among pregnant people immediately postpartum, but evidence suggests these relapses may related to lack of follow-up care after an initial treatment episode during pregnancy. For instance, some discontinue opioid use disorder care postpartum due to mental health problems. There is a need to understand how to engage pregnant people more effectively in care throughout the pregnancy process, including after birth. This engagement might ideally consider the barriers pregnant people with substance use disorders face in receiving care (e.g., stigma, lack of treatment options and difficulties enrolling in care). To this end, the present study tested the feasibility of a patient-navigation based intervention designed to help pregnant people overcome barriers to care as well as achieve and maintain opioid abstinence postpartum.
HOW WAS THIS STUDY CONDUCTED?
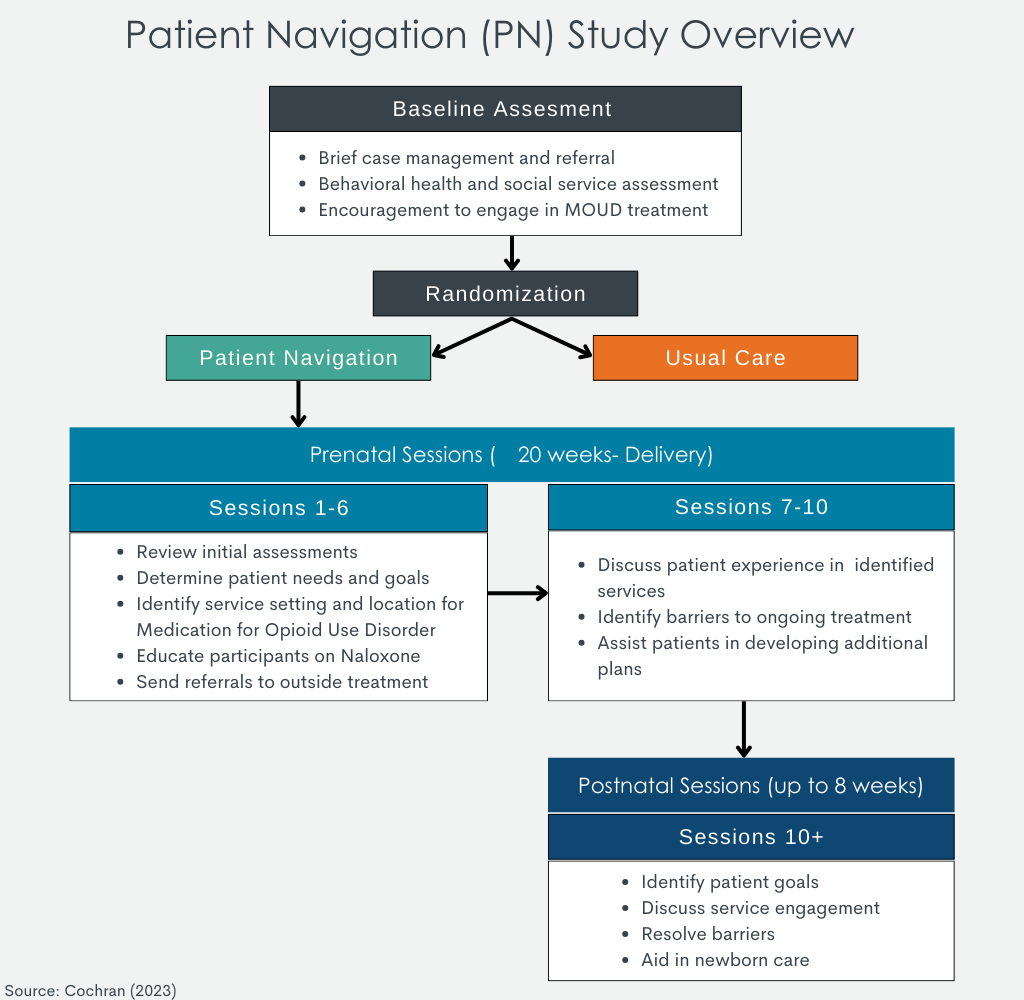
This study was a single-blinded randomized controlled trial with staff conducting outcome assessments unaware of (i.e., “blind” to) study condition. Participants were 102 patients at two academic medical centers in different parts of the US: western Pennsylvania, and central Utah. Pregnant people enrolled in the study were asked to complete a baseline assessment, followed by up to 10 intervention sessions. A post-intervention follow-up assessment was then conducted before the individual gave birth (8–14 weeks post-baseline depending upon participants’ remaining prepartum time) as well as 2 and 6 months after giving birth (i.e., postnatally). Sessions lasted 30–60 minutes each and focused on substance use, mental health, medical or social service needs (including naloxone training and referral).
Potential participants were identified through medical record screening. Eligibility criteria included: 1) greater than 7 weeks’ gestation (confirmed via ultrasound) and 2) meeting DSM-5 criteria for an opioid use disorder. Participants were excluded from participation if they: a) had been taking medications for opioid use disorder for > 6 weeks (given the study focus is on helping patients initiate and sustain treatment engagement) b) self-reported psychosis or mania c) beyond 32 weeks’ gestation d) planned pregnancy termination, e) inadequate contact information for themselves or two collateral sources, f) lack of a working telephone g) or planned relocation during the study.
The study (titled OPTI-Mom v 2.0) tested the feasibility of a patient navigation-based intervention designed to improve opioid disorder outcomes among pregnant people with an opioid use disorder. Patient navigation is a behavioral intervention approach which focuses on helping patients navigate medical care systems and remain in care. Patient navigation does this by addressing barriers to care which prevent patients from accessing needs. These barriers include psychological factors like fear/anxiety around treatment seeking and issues with patient-provider communications. Barriers can also be external (e.g., financial and/or transportation limitations). This form of intervention entails patient navigators and patients developing close one-to-one bonds, whereby the navigator comes to understand the specific individual needs of the patient. Patient navigation is similar to recovery coaching, but where personal experience with addiction and recovery is not the norm as is the case for recovery coaching. In this study patient navigators were masters-level research clinicians who received specialized training in motivational interviewing and monthly supervision from a licensed counselor.
All participants received usual care at initiation of the study procedures. These entailed participants meeting briefly with a social worker which conducted a behavioral health and social services assessment. The social worker provided written referrals to agencies and/or other clinical services for these patients. All patients were provided with referrals for opioid use disorder medication for treatment. In addition to this usual care, those who received the patient navigation intervention also met with patient navigators pre- and postpartum (see intervention description below).
The primary outcome of this study was to assess the feasibility of the intervention across study sites (Pennsylvania and Utah). This was determined via percentages of patients approached who consented to participate, number of sessions administered to participants in the patient navigation condition, and assessment completion rates, as well as engagement and retention in opioid use disorder treatment. The primary treatment engagement outcome was percent days taking an FDA-approved opioid use disorder medication (e.g., buprenorphine often prescribed in formulation known by the brand name Suboxone or extended-release naltrexone also known by the brand name Vivitrol). Secondary treatment engagement outcomes were percent days attending outpatient or inpatient substance use disorder treatment. The researchers were also interested in prenatal care engagement, which they measured via the Prenatal Care Utilization index. This validated tool classifies prenatal care into adequate plus, adequate, intermediate, and inadequate categories. Finally, the study sought to determine how the intervention impacted the incidence of non-medical (i.e., non-prescribed) opioid use among participants postpartum. The study used the timeline follow-back to assess both treatment engagement and non-medical opioid use.
Analyses examined group differences (i.e., the patient-navigation condition vs. usual care) on changes in outcomes from baseline to follow-ups. Separate models were run to include participants who completed at least 6 prenatal sessions (i.e., “per-protocol” sample) and all participants who were assigned to a study condition regardless of the number of sessions they completed (i.e., “intent-to-treat” sample). The researchers emphasized the magnitude of the group difference rather than how “reliable” this effect might be (i.e., whether it was statistically significant), a common approach for studies like these at the pilot stage.
Participants in the sample were fairly evenly split between the study sites, with 44.1% and 55.9% coming from Utah and Pennsylvania respectively. Most participants were 25-34 years of age (70.6%). Most of the sample was White (83.3%) and did not identify as Hispanic/Latina (93.1%). Most of the sample had at a high school education (64.7%), was employed (52.9%), and was not married (75.5%). Most of the sample had at least 1 child already at baseline assessment (74.5%).
WHAT DID THIS STUDY FIND?
The patient navigation intervention was feasible
Of the 134 potentially eligible participants, 106 consented to participate. Of these, 102 were randomized to either the intervention or usual care. Of the 53 who received the patient navigation intervention, 88% completed both the baseline and prenatal assessment. The median number of sessions completed by participants was 6 (out of 10). Furthermore, 75% completed the 2-month postnatal assessment and 87% completed the 6-month postnatal assessment.
The patient navigation and usual care groups both engaged in opioid use disorder treatment
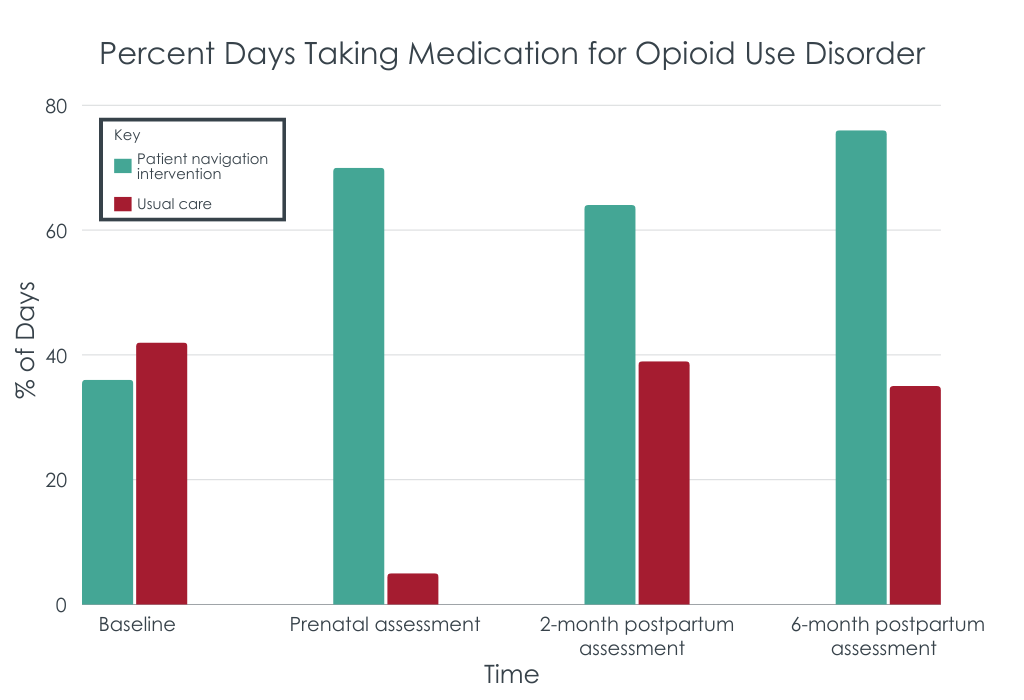
Increases in substance use disorder treatment attendance was higher among participants who received patient navigation than those who received usual care, especially for opioid use disorder medications. The greater improvements in the patient navigation group did not reach statistical significance; but, for example, from baseline to the prenatal assessment, the patient navigation group had an increase of 40% of days taking medication compared to an increase of 30% in the usual care group (see figure below).
The patient navigation group had better opioid use outcomes
Postpartum, those who received patient navigation reported greater decreases in non-medical opioid use than those receiving usual care. For example, at the 6-month follow-up, the patient navigation group had 56% fewer days of opioid use relative to baseline compared to 48% fewer days of opioid use in usual care relative to baseline. Like the treatment engagement outcomes above, these greater decreases in opioid use were consistent over time but did not reach statistical significance. At all times during the study, participants receiving patient navigation reported fewer overdoses than those who received usual care.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that patient navigation can be a feasible way to facilitate opioid use disorder care participation among pregnant people in the US. The researchers found that 3/4 of those who were eligible consented to participate, the average participant received a full “dose” of treatment, and nearly 9 in 10 completed the 6-month postnatal assessment (i.e., the final follow-up). Taken together, these results suggest that the patient navigation condition may have high adoptability in real-world settings.
The results of this study also suggest that the patient navigation intervention has the potential to improve participant treatment engagement and opioid use outcomes. Given the early stages of the intervention, the study was not designed to test for statistical significance, i.e., a reliable difference. That said, participants in the patient navigation condition had greater improvements in opioid use disorder care attendance and opioid use outcomes than those who were simply referred to treatment, although the magnitude of the advantage was modest.
Overall, the current results suggest that a patient navigation intervention can be feasibly implemented across multiple healthcare settings. Further research is needed to determine the relative efficacy of the intervention compared to other strategies also designed to facilitate participation in treatment, such as recovery coaching.
The study took place between April 2019 and February 2022, meaning that a number of participants were recruited during the COVID-19 pandemic. This is an issue as it is unclear whether disruptions in healthcare may have impacted the study results. That is, it is plausible that fear of COVID-19 infection may have resulted in participants minimizing unnecessary contact with healthcare personnel which may have resulted in lower study recruitment. Alternatively, if remote sessions were offered (e.g., through telemedicine) this may have facilitated study enrollment and thus inflated feasibility metrics. The authors do not discuss how the intervention procedures were administered (e.g., in person or remote) nor how the study was impacted by the COVID-19 pandemic.
The results suggest that the effectiveness of the intervention may have varied across study sites. Although the analyses yielded no statistically significant differences in behavioral outcomes when examining the entire sample, subgroup analyses did find that participants in Utah attended significantly more treatment appointments and used more medication to treat opioid use disorder than participants in Pennsylvania. It is unknown why these differences arose between study locations. It is possible that regional variances in culture (e.g., the higher proportion of Church of Latter-Day Saints members in Utah relative to other states) may have impacted the efficacy of the intervention Utah may be stronger with social/community ties vis-a-vis Church membership aided in recovery for participants there. Future research may benefit from accounting for cultural contexts in different US regions.
BOTTOM LINE
Results suggest that patient navigation-based interventions can be feasibly implemented in healthcare settings and may be somewhat efficacious at improving treatment engagement and opioid use outcomes among pregnant people with opioid use disorders. Although these differences failed to reach significance, they suggest adding patient navigators to the health care teams of pregnant and postpartum people with opioid use disorder, which may improve outcomes. Further research is needed to expand upon these findings and offer more concrete evidence for the impact of patient navigation on health outcomes among pregnant people with an opioid use disorder.
For individuals and families seeking recovery: Patient navigation-based interventions may be an effective strategy to address the barriers which hamper pregnant people’s ability to receive and remain in opioid use disorder treatment. However, given that this was a pilot study, more research is needed before recommendations can be made.
For treatment professionals and treatment systems: The present study suggests that patient navigation can help pregnant people in the US overcome barriers to accessing and staying in opioid use disorder treatment. Those providing treatment to and/or work in healthcare system settings serving these populations may consider ways to incorporate patient navigation techniques and/or minimize the potential burdens among patients. For example, integrating telemedicine more into their practices may relieve some of the childcare burden faced by those in treatment who have children.
For scientists: Further work is needed to determine the relative effectiveness of patient navigation interventions in linking and maintaining pregnant people in opioid use disorder treatment. Barriers to care clearly exist, (e.g., perceived stigma of opioid use disorder and health insurance) and therefore it seems plausible patient navigation (with its focus on addressing individually relevant barriers to care) could be an effective intervention. Nevertheless, the present study was underpowered to determine treatment effects. Therefore, scientists would do well to scale up this work and conduct larger scale randomized control clinical trial research testing the effect of patient navigation on health outcomes.
For policy makers: The present research suggests that patient navigation may be a viable tool for increasing treatment usage and retention among pregnant people who have opioid use disorders. This suggests that policy makers could improve treatment outcomes by addressing some of the barriers to care for this population. That is, patient navigation is predicated on the fact that treatment access is disproportionately more challenging for some populations than others. Increasing healthcare access (e.g., increase public clinics serving communities) may be one approach to lowering these barriers. However, given that this was a pilot study, more research is needed to inform best practice policies and guidelines for patient navigation among pregnant people with opioid use disorders.
It is unclear why relapse rates are so high among pregnant people immediately postpartum, but evidence suggests these relapses may related to lack of follow-up care after an initial treatment episode during pregnancy. For instance, some discontinue opioid use disorder care postpartum due to mental health problems. There is a need to understand how to engage pregnant people more effectively in care throughout the pregnancy process, including after birth. This engagement might ideally consider the barriers pregnant people with substance use disorders face in receiving care (e.g., stigma, lack of treatment options and difficulties enrolling in care). To this end, the present study tested the feasibility of a patient-navigation based intervention designed to help pregnant people overcome barriers to care as well as achieve and maintain opioid abstinence postpartum.
HOW WAS THIS STUDY CONDUCTED?
This study was a single-blinded randomized controlled trial with staff conducting outcome assessments unaware of (i.e., “blind” to) study condition. Participants were 102 patients at two academic medical centers in different parts of the US: western Pennsylvania, and central Utah. Pregnant people enrolled in the study were asked to complete a baseline assessment, followed by up to 10 intervention sessions. A post-intervention follow-up assessment was then conducted before the individual gave birth (8–14 weeks post-baseline depending upon participants’ remaining prepartum time) as well as 2 and 6 months after giving birth (i.e., postnatally). Sessions lasted 30–60 minutes each and focused on substance use, mental health, medical or social service needs (including naloxone training and referral).
Potential participants were identified through medical record screening. Eligibility criteria included: 1) greater than 7 weeks’ gestation (confirmed via ultrasound) and 2) meeting DSM-5 criteria for an opioid use disorder. Participants were excluded from participation if they: a) had been taking medications for opioid use disorder for > 6 weeks (given the study focus is on helping patients initiate and sustain treatment engagement) b) self-reported psychosis or mania c) beyond 32 weeks’ gestation d) planned pregnancy termination, e) inadequate contact information for themselves or two collateral sources, f) lack of a working telephone g) or planned relocation during the study.
The study (titled OPTI-Mom v 2.0) tested the feasibility of a patient navigation-based intervention designed to improve opioid disorder outcomes among pregnant people with an opioid use disorder. Patient navigation is a behavioral intervention approach which focuses on helping patients navigate medical care systems and remain in care. Patient navigation does this by addressing barriers to care which prevent patients from accessing needs. These barriers include psychological factors like fear/anxiety around treatment seeking and issues with patient-provider communications. Barriers can also be external (e.g., financial and/or transportation limitations). This form of intervention entails patient navigators and patients developing close one-to-one bonds, whereby the navigator comes to understand the specific individual needs of the patient. Patient navigation is similar to recovery coaching, but where personal experience with addiction and recovery is not the norm as is the case for recovery coaching. In this study patient navigators were masters-level research clinicians who received specialized training in motivational interviewing and monthly supervision from a licensed counselor.
All participants received usual care at initiation of the study procedures. These entailed participants meeting briefly with a social worker which conducted a behavioral health and social services assessment. The social worker provided written referrals to agencies and/or other clinical services for these patients. All patients were provided with referrals for opioid use disorder medication for treatment. In addition to this usual care, those who received the patient navigation intervention also met with patient navigators pre- and postpartum (see intervention description below).
The primary outcome of this study was to assess the feasibility of the intervention across study sites (Pennsylvania and Utah). This was determined via percentages of patients approached who consented to participate, number of sessions administered to participants in the patient navigation condition, and assessment completion rates, as well as engagement and retention in opioid use disorder treatment. The primary treatment engagement outcome was percent days taking an FDA-approved opioid use disorder medication (e.g., buprenorphine often prescribed in formulation known by the brand name Suboxone or extended-release naltrexone also known by the brand name Vivitrol). Secondary treatment engagement outcomes were percent days attending outpatient or inpatient substance use disorder treatment. The researchers were also interested in prenatal care engagement, which they measured via the Prenatal Care Utilization index. This validated tool classifies prenatal care into adequate plus, adequate, intermediate, and inadequate categories. Finally, the study sought to determine how the intervention impacted the incidence of non-medical (i.e., non-prescribed) opioid use among participants postpartum. The study used the timeline follow-back to assess both treatment engagement and non-medical opioid use.
Analyses examined group differences (i.e., the patient-navigation condition vs. usual care) on changes in outcomes from baseline to follow-ups. Separate models were run to include participants who completed at least 6 prenatal sessions (i.e., “per-protocol” sample) and all participants who were assigned to a study condition regardless of the number of sessions they completed (i.e., “intent-to-treat” sample). The researchers emphasized the magnitude of the group difference rather than how “reliable” this effect might be (i.e., whether it was statistically significant), a common approach for studies like these at the pilot stage.
Participants in the sample were fairly evenly split between the study sites, with 44.1% and 55.9% coming from Utah and Pennsylvania respectively. Most participants were 25-34 years of age (70.6%). Most of the sample was White (83.3%) and did not identify as Hispanic/Latina (93.1%). Most of the sample had at a high school education (64.7%), was employed (52.9%), and was not married (75.5%). Most of the sample had at least 1 child already at baseline assessment (74.5%).
WHAT DID THIS STUDY FIND?
The patient navigation intervention was feasible
Of the 134 potentially eligible participants, 106 consented to participate. Of these, 102 were randomized to either the intervention or usual care. Of the 53 who received the patient navigation intervention, 88% completed both the baseline and prenatal assessment. The median number of sessions completed by participants was 6 (out of 10). Furthermore, 75% completed the 2-month postnatal assessment and 87% completed the 6-month postnatal assessment.
The patient navigation and usual care groups both engaged in opioid use disorder treatment
Increases in substance use disorder treatment attendance was higher among participants who received patient navigation than those who received usual care, especially for opioid use disorder medications. The greater improvements in the patient navigation group did not reach statistical significance; but, for example, from baseline to the prenatal assessment, the patient navigation group had an increase of 40% of days taking medication compared to an increase of 30% in the usual care group (see figure below).
The patient navigation group had better opioid use outcomes
Postpartum, those who received patient navigation reported greater decreases in non-medical opioid use than those receiving usual care. For example, at the 6-month follow-up, the patient navigation group had 56% fewer days of opioid use relative to baseline compared to 48% fewer days of opioid use in usual care relative to baseline. Like the treatment engagement outcomes above, these greater decreases in opioid use were consistent over time but did not reach statistical significance. At all times during the study, participants receiving patient navigation reported fewer overdoses than those who received usual care.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that patient navigation can be a feasible way to facilitate opioid use disorder care participation among pregnant people in the US. The researchers found that 3/4 of those who were eligible consented to participate, the average participant received a full “dose” of treatment, and nearly 9 in 10 completed the 6-month postnatal assessment (i.e., the final follow-up). Taken together, these results suggest that the patient navigation condition may have high adoptability in real-world settings.
The results of this study also suggest that the patient navigation intervention has the potential to improve participant treatment engagement and opioid use outcomes. Given the early stages of the intervention, the study was not designed to test for statistical significance, i.e., a reliable difference. That said, participants in the patient navigation condition had greater improvements in opioid use disorder care attendance and opioid use outcomes than those who were simply referred to treatment, although the magnitude of the advantage was modest.
Overall, the current results suggest that a patient navigation intervention can be feasibly implemented across multiple healthcare settings. Further research is needed to determine the relative efficacy of the intervention compared to other strategies also designed to facilitate participation in treatment, such as recovery coaching.
The study took place between April 2019 and February 2022, meaning that a number of participants were recruited during the COVID-19 pandemic. This is an issue as it is unclear whether disruptions in healthcare may have impacted the study results. That is, it is plausible that fear of COVID-19 infection may have resulted in participants minimizing unnecessary contact with healthcare personnel which may have resulted in lower study recruitment. Alternatively, if remote sessions were offered (e.g., through telemedicine) this may have facilitated study enrollment and thus inflated feasibility metrics. The authors do not discuss how the intervention procedures were administered (e.g., in person or remote) nor how the study was impacted by the COVID-19 pandemic.
The results suggest that the effectiveness of the intervention may have varied across study sites. Although the analyses yielded no statistically significant differences in behavioral outcomes when examining the entire sample, subgroup analyses did find that participants in Utah attended significantly more treatment appointments and used more medication to treat opioid use disorder than participants in Pennsylvania. It is unknown why these differences arose between study locations. It is possible that regional variances in culture (e.g., the higher proportion of Church of Latter-Day Saints members in Utah relative to other states) may have impacted the efficacy of the intervention Utah may be stronger with social/community ties vis-a-vis Church membership aided in recovery for participants there. Future research may benefit from accounting for cultural contexts in different US regions.
BOTTOM LINE
Results suggest that patient navigation-based interventions can be feasibly implemented in healthcare settings and may be somewhat efficacious at improving treatment engagement and opioid use outcomes among pregnant people with opioid use disorders. Although these differences failed to reach significance, they suggest adding patient navigators to the health care teams of pregnant and postpartum people with opioid use disorder, which may improve outcomes. Further research is needed to expand upon these findings and offer more concrete evidence for the impact of patient navigation on health outcomes among pregnant people with an opioid use disorder.
For individuals and families seeking recovery: Patient navigation-based interventions may be an effective strategy to address the barriers which hamper pregnant people’s ability to receive and remain in opioid use disorder treatment. However, given that this was a pilot study, more research is needed before recommendations can be made.
For treatment professionals and treatment systems: The present study suggests that patient navigation can help pregnant people in the US overcome barriers to accessing and staying in opioid use disorder treatment. Those providing treatment to and/or work in healthcare system settings serving these populations may consider ways to incorporate patient navigation techniques and/or minimize the potential burdens among patients. For example, integrating telemedicine more into their practices may relieve some of the childcare burden faced by those in treatment who have children.
For scientists: Further work is needed to determine the relative effectiveness of patient navigation interventions in linking and maintaining pregnant people in opioid use disorder treatment. Barriers to care clearly exist, (e.g., perceived stigma of opioid use disorder and health insurance) and therefore it seems plausible patient navigation (with its focus on addressing individually relevant barriers to care) could be an effective intervention. Nevertheless, the present study was underpowered to determine treatment effects. Therefore, scientists would do well to scale up this work and conduct larger scale randomized control clinical trial research testing the effect of patient navigation on health outcomes.
For policy makers: The present research suggests that patient navigation may be a viable tool for increasing treatment usage and retention among pregnant people who have opioid use disorders. This suggests that policy makers could improve treatment outcomes by addressing some of the barriers to care for this population. That is, patient navigation is predicated on the fact that treatment access is disproportionately more challenging for some populations than others. Increasing healthcare access (e.g., increase public clinics serving communities) may be one approach to lowering these barriers. However, given that this was a pilot study, more research is needed to inform best practice policies and guidelines for patient navigation among pregnant people with opioid use disorders.
It is unclear why relapse rates are so high among pregnant people immediately postpartum, but evidence suggests these relapses may related to lack of follow-up care after an initial treatment episode during pregnancy. For instance, some discontinue opioid use disorder care postpartum due to mental health problems. There is a need to understand how to engage pregnant people more effectively in care throughout the pregnancy process, including after birth. This engagement might ideally consider the barriers pregnant people with substance use disorders face in receiving care (e.g., stigma, lack of treatment options and difficulties enrolling in care). To this end, the present study tested the feasibility of a patient-navigation based intervention designed to help pregnant people overcome barriers to care as well as achieve and maintain opioid abstinence postpartum.
HOW WAS THIS STUDY CONDUCTED?
This study was a single-blinded randomized controlled trial with staff conducting outcome assessments unaware of (i.e., “blind” to) study condition. Participants were 102 patients at two academic medical centers in different parts of the US: western Pennsylvania, and central Utah. Pregnant people enrolled in the study were asked to complete a baseline assessment, followed by up to 10 intervention sessions. A post-intervention follow-up assessment was then conducted before the individual gave birth (8–14 weeks post-baseline depending upon participants’ remaining prepartum time) as well as 2 and 6 months after giving birth (i.e., postnatally). Sessions lasted 30–60 minutes each and focused on substance use, mental health, medical or social service needs (including naloxone training and referral).
Potential participants were identified through medical record screening. Eligibility criteria included: 1) greater than 7 weeks’ gestation (confirmed via ultrasound) and 2) meeting DSM-5 criteria for an opioid use disorder. Participants were excluded from participation if they: a) had been taking medications for opioid use disorder for > 6 weeks (given the study focus is on helping patients initiate and sustain treatment engagement) b) self-reported psychosis or mania c) beyond 32 weeks’ gestation d) planned pregnancy termination, e) inadequate contact information for themselves or two collateral sources, f) lack of a working telephone g) or planned relocation during the study.
The study (titled OPTI-Mom v 2.0) tested the feasibility of a patient navigation-based intervention designed to improve opioid disorder outcomes among pregnant people with an opioid use disorder. Patient navigation is a behavioral intervention approach which focuses on helping patients navigate medical care systems and remain in care. Patient navigation does this by addressing barriers to care which prevent patients from accessing needs. These barriers include psychological factors like fear/anxiety around treatment seeking and issues with patient-provider communications. Barriers can also be external (e.g., financial and/or transportation limitations). This form of intervention entails patient navigators and patients developing close one-to-one bonds, whereby the navigator comes to understand the specific individual needs of the patient. Patient navigation is similar to recovery coaching, but where personal experience with addiction and recovery is not the norm as is the case for recovery coaching. In this study patient navigators were masters-level research clinicians who received specialized training in motivational interviewing and monthly supervision from a licensed counselor.
All participants received usual care at initiation of the study procedures. These entailed participants meeting briefly with a social worker which conducted a behavioral health and social services assessment. The social worker provided written referrals to agencies and/or other clinical services for these patients. All patients were provided with referrals for opioid use disorder medication for treatment. In addition to this usual care, those who received the patient navigation intervention also met with patient navigators pre- and postpartum (see intervention description below).
The primary outcome of this study was to assess the feasibility of the intervention across study sites (Pennsylvania and Utah). This was determined via percentages of patients approached who consented to participate, number of sessions administered to participants in the patient navigation condition, and assessment completion rates, as well as engagement and retention in opioid use disorder treatment. The primary treatment engagement outcome was percent days taking an FDA-approved opioid use disorder medication (e.g., buprenorphine often prescribed in formulation known by the brand name Suboxone or extended-release naltrexone also known by the brand name Vivitrol). Secondary treatment engagement outcomes were percent days attending outpatient or inpatient substance use disorder treatment. The researchers were also interested in prenatal care engagement, which they measured via the Prenatal Care Utilization index. This validated tool classifies prenatal care into adequate plus, adequate, intermediate, and inadequate categories. Finally, the study sought to determine how the intervention impacted the incidence of non-medical (i.e., non-prescribed) opioid use among participants postpartum. The study used the timeline follow-back to assess both treatment engagement and non-medical opioid use.
Analyses examined group differences (i.e., the patient-navigation condition vs. usual care) on changes in outcomes from baseline to follow-ups. Separate models were run to include participants who completed at least 6 prenatal sessions (i.e., “per-protocol” sample) and all participants who were assigned to a study condition regardless of the number of sessions they completed (i.e., “intent-to-treat” sample). The researchers emphasized the magnitude of the group difference rather than how “reliable” this effect might be (i.e., whether it was statistically significant), a common approach for studies like these at the pilot stage.
Participants in the sample were fairly evenly split between the study sites, with 44.1% and 55.9% coming from Utah and Pennsylvania respectively. Most participants were 25-34 years of age (70.6%). Most of the sample was White (83.3%) and did not identify as Hispanic/Latina (93.1%). Most of the sample had at a high school education (64.7%), was employed (52.9%), and was not married (75.5%). Most of the sample had at least 1 child already at baseline assessment (74.5%).
WHAT DID THIS STUDY FIND?
The patient navigation intervention was feasible
Of the 134 potentially eligible participants, 106 consented to participate. Of these, 102 were randomized to either the intervention or usual care. Of the 53 who received the patient navigation intervention, 88% completed both the baseline and prenatal assessment. The median number of sessions completed by participants was 6 (out of 10). Furthermore, 75% completed the 2-month postnatal assessment and 87% completed the 6-month postnatal assessment.
The patient navigation and usual care groups both engaged in opioid use disorder treatment
Increases in substance use disorder treatment attendance was higher among participants who received patient navigation than those who received usual care, especially for opioid use disorder medications. The greater improvements in the patient navigation group did not reach statistical significance; but, for example, from baseline to the prenatal assessment, the patient navigation group had an increase of 40% of days taking medication compared to an increase of 30% in the usual care group (see figure below).
The patient navigation group had better opioid use outcomes
Postpartum, those who received patient navigation reported greater decreases in non-medical opioid use than those receiving usual care. For example, at the 6-month follow-up, the patient navigation group had 56% fewer days of opioid use relative to baseline compared to 48% fewer days of opioid use in usual care relative to baseline. Like the treatment engagement outcomes above, these greater decreases in opioid use were consistent over time but did not reach statistical significance. At all times during the study, participants receiving patient navigation reported fewer overdoses than those who received usual care.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that patient navigation can be a feasible way to facilitate opioid use disorder care participation among pregnant people in the US. The researchers found that 3/4 of those who were eligible consented to participate, the average participant received a full “dose” of treatment, and nearly 9 in 10 completed the 6-month postnatal assessment (i.e., the final follow-up). Taken together, these results suggest that the patient navigation condition may have high adoptability in real-world settings.
The results of this study also suggest that the patient navigation intervention has the potential to improve participant treatment engagement and opioid use outcomes. Given the early stages of the intervention, the study was not designed to test for statistical significance, i.e., a reliable difference. That said, participants in the patient navigation condition had greater improvements in opioid use disorder care attendance and opioid use outcomes than those who were simply referred to treatment, although the magnitude of the advantage was modest.
Overall, the current results suggest that a patient navigation intervention can be feasibly implemented across multiple healthcare settings. Further research is needed to determine the relative efficacy of the intervention compared to other strategies also designed to facilitate participation in treatment, such as recovery coaching.
The study took place between April 2019 and February 2022, meaning that a number of participants were recruited during the COVID-19 pandemic. This is an issue as it is unclear whether disruptions in healthcare may have impacted the study results. That is, it is plausible that fear of COVID-19 infection may have resulted in participants minimizing unnecessary contact with healthcare personnel which may have resulted in lower study recruitment. Alternatively, if remote sessions were offered (e.g., through telemedicine) this may have facilitated study enrollment and thus inflated feasibility metrics. The authors do not discuss how the intervention procedures were administered (e.g., in person or remote) nor how the study was impacted by the COVID-19 pandemic.
The results suggest that the effectiveness of the intervention may have varied across study sites. Although the analyses yielded no statistically significant differences in behavioral outcomes when examining the entire sample, subgroup analyses did find that participants in Utah attended significantly more treatment appointments and used more medication to treat opioid use disorder than participants in Pennsylvania. It is unknown why these differences arose between study locations. It is possible that regional variances in culture (e.g., the higher proportion of Church of Latter-Day Saints members in Utah relative to other states) may have impacted the efficacy of the intervention Utah may be stronger with social/community ties vis-a-vis Church membership aided in recovery for participants there. Future research may benefit from accounting for cultural contexts in different US regions.
BOTTOM LINE
Results suggest that patient navigation-based interventions can be feasibly implemented in healthcare settings and may be somewhat efficacious at improving treatment engagement and opioid use outcomes among pregnant people with opioid use disorders. Although these differences failed to reach significance, they suggest adding patient navigators to the health care teams of pregnant and postpartum people with opioid use disorder, which may improve outcomes. Further research is needed to expand upon these findings and offer more concrete evidence for the impact of patient navigation on health outcomes among pregnant people with an opioid use disorder.
For individuals and families seeking recovery: Patient navigation-based interventions may be an effective strategy to address the barriers which hamper pregnant people’s ability to receive and remain in opioid use disorder treatment. However, given that this was a pilot study, more research is needed before recommendations can be made.
For treatment professionals and treatment systems: The present study suggests that patient navigation can help pregnant people in the US overcome barriers to accessing and staying in opioid use disorder treatment. Those providing treatment to and/or work in healthcare system settings serving these populations may consider ways to incorporate patient navigation techniques and/or minimize the potential burdens among patients. For example, integrating telemedicine more into their practices may relieve some of the childcare burden faced by those in treatment who have children.
For scientists: Further work is needed to determine the relative effectiveness of patient navigation interventions in linking and maintaining pregnant people in opioid use disorder treatment. Barriers to care clearly exist, (e.g., perceived stigma of opioid use disorder and health insurance) and therefore it seems plausible patient navigation (with its focus on addressing individually relevant barriers to care) could be an effective intervention. Nevertheless, the present study was underpowered to determine treatment effects. Therefore, scientists would do well to scale up this work and conduct larger scale randomized control clinical trial research testing the effect of patient navigation on health outcomes.
For policy makers: The present research suggests that patient navigation may be a viable tool for increasing treatment usage and retention among pregnant people who have opioid use disorders. This suggests that policy makers could improve treatment outcomes by addressing some of the barriers to care for this population. That is, patient navigation is predicated on the fact that treatment access is disproportionately more challenging for some populations than others. Increasing healthcare access (e.g., increase public clinics serving communities) may be one approach to lowering these barriers. However, given that this was a pilot study, more research is needed to inform best practice policies and guidelines for patient navigation among pregnant people with opioid use disorders.


 Analyses examined group differences (i.e., the patient-navigation condition vs. usual care) on changes in outcomes from baseline to follow-ups. Separate models were run to include participants who completed at least 6 prenatal sessions (i.e., “per-protocol” sample) and all participants who were assigned to a study condition regardless of the number of sessions they completed (i.e., “intent-to-treat” sample). The researchers emphasized the magnitude of the group difference rather than how “reliable” this effect might be (i.e., whether it was statistically significant), a common approach for studies like these at the pilot stage.
Analyses examined group differences (i.e., the patient-navigation condition vs. usual care) on changes in outcomes from baseline to follow-ups. Separate models were run to include participants who completed at least 6 prenatal sessions (i.e., “per-protocol” sample) and all participants who were assigned to a study condition regardless of the number of sessions they completed (i.e., “intent-to-treat” sample). The researchers emphasized the magnitude of the group difference rather than how “reliable” this effect might be (i.e., whether it was statistically significant), a common approach for studies like these at the pilot stage.