Improving treatment retention? Examining the move from daily to once per month injectable buprenorphine
Buprenorphine is a helpful medication in treating opioid use disorder but treatment retention is an ongoing barrier to successful recovery. Once per month injectable extended-release buprenorphine formulations may help ease retention challenges, but little is known about its utility particularly when individuals transition from oral daily buprenorphine to the once per month injectable formulation. This study investigated real-world retention rates and clinical predictors of retention in patients transitioning from long-term treatment with daily dosed sublingual buprenorphine to the long-acting once per month injectable extended-release injectable version.
Buprenorphine is a helpful medication for opioid use disorder, reducing opioid craving, misuse, and overdose risk. Sublingual buprenorphine was approved for opioid use disorder treatment in the United States in 2002 and is now the most commonly prescribed pharmacotherapy for the disorder. Because this form of the medication is taken daily and prescribed in office-based settings, there are concerns around medication adherence and treatment retention. About two-thirds of individuals stop taking their medication within six months of treatment, which increases risk of returning to illicit opioid use and overdosing. The need to dose daily and attend frequent office-based doctor visits to renew sublingual buprenorphine prescriptions might contribute to adherence and retention issues. Thus, long-acting injectable extended-release versions of the medication might help. Long-acting versions of another FDA approved medication in the treatment of opioid use disorder – long-acting naltrexone (sold under the brand Vivitrol) has shown helpful in increasing abstinence from illicit opioids and such long-acting variants of these medications may be particularly helpful for certain groups of people, such as those experiencing homelessness, who have been shown to have better outcomes on the extended release formulation of naltrexone (Vivitrol), compared to daily buprenorphine.
An extended-release injectable formulation of buprenorphine was approved in 2017 and is as safe and effective as sublingual formulations. This once monthly injectable requires fewer office visits and helps to prevent compliance issues seen with daily dosing. However, few studies have examined real-world treatment retention with injectable extended-release buprenorphine or patient characteristics that might influence it. Even fewer studies have evaluated retention among those who are transitioning to extended-release buprenorphine after longer-term daily dosed buprenorphine. Research on extended-release injectable buprenorphine can help improve opioid use disorder treatment recommendations. The current study examined real-world retention rates in patients transitioning from longer-term daily dosing to the injectable version, as well as factors that predict successful retention after transitioning.
HOW WAS THIS STUDY CONDUCTED?
The study examined electronic medical records to estimate 6-month retention on injectable extended-release buprenorphine in 92 consecutive patients with opioid use disorder who transitioned from sublingual (i.e., often prescribed in formulation with naloxone known by the brand name Suboxone) to injectable buprenorphine (i.e. of which Sublocade is one brand name formulation).
All participants were patients from a single treatment facility in Massachusetts who were stabilized on sublingual buprenorphine (8-24 mg per day) and had insurance that covered reimbursement for extended-release buprenorphine treatment.
Patients had been on sublingual buprenorphine for an average of 17 months and received their first extended-release buprenorphine injection between 2018 and 2019. In general, the first two injections (months 1 and 2) were 300 mg doses and subsequent injections (month 3 and later) were 100 mg doses. However, patients who experienced withdrawal or craving were supplemented with low doses (2-4 mg per day) of sublingual buprenorphine during the first two months of extended-release injectable buprenorphine treatment, and those who continued to experience withdrawal or craving at month 3 and beyond continued to receive 300 mg injections (instead of reducing to 100 mg).
Retention rate was examined as the proportion of individuals who received 0, 1, 2, and 3 or more follow-up injections within six months of their initial injection. Demographics, substance use history, and treatment history were also obtained from the medical records and the researchers examined whether these variables differed between patients who received 3 or more follow-up injections – the marker of “successful” retention in the current study – relative to those who received less than 3 doses.
The majority of participants were white (90%) men (67%) in their late thirties (average age of 38 years) with a history of injection drug use (73%). About 40% used heroin in the three months prior to their first buprenorphine injection. In terms of other current diagnoses, 34% had a chronic pain diagnosis and 67% had a comorbid psychiatric disorder (e.g., major depression, bipolar disorder, anxiety disorder, psychotic disorder).
WHAT DID THIS STUDY FIND?
About half of the patients were successfully retained on extended-release injectable buprenorphine.
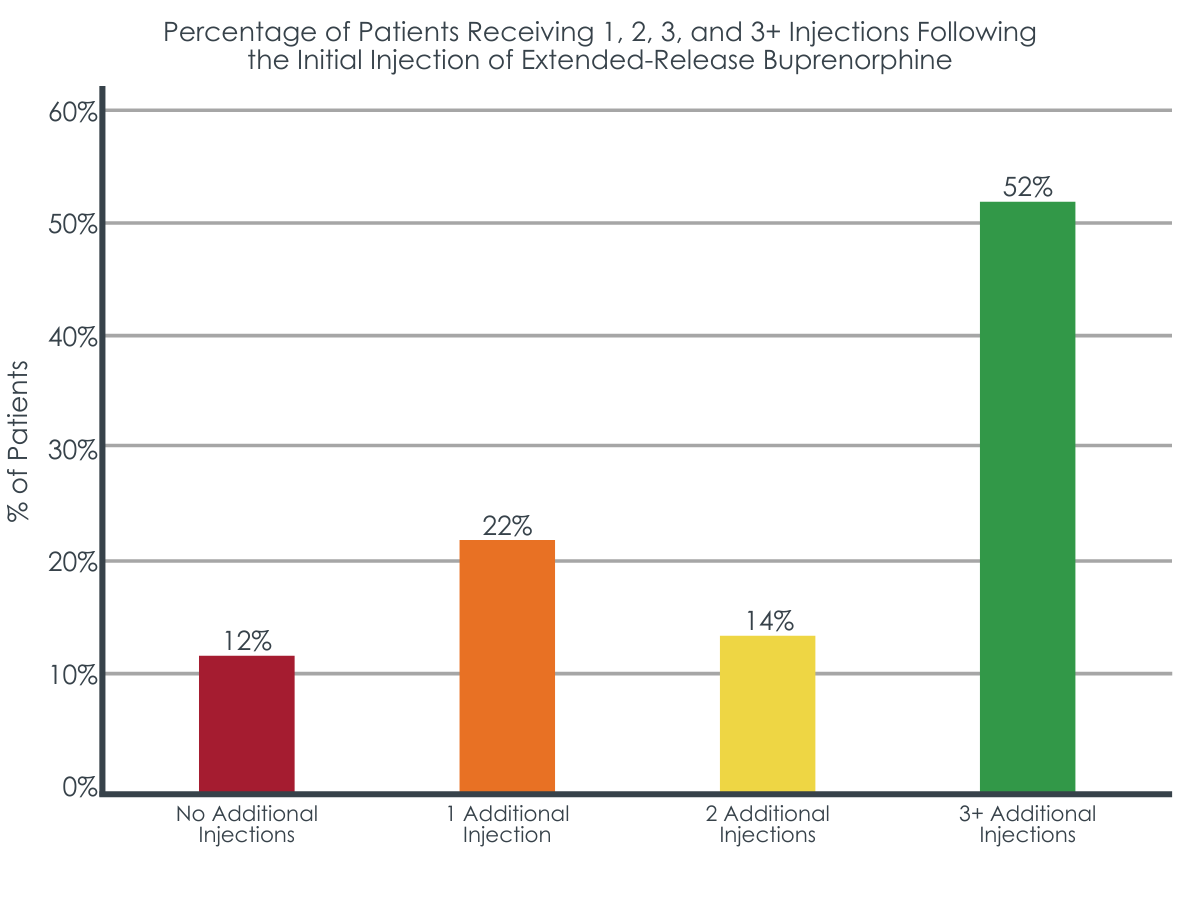
Fifty-two percent of patients received three or more extended-release buprenorphine injections after their initial injection. Thirty-six percent of patients received one or two follow-up doses and 12% discontinued treatment after the first dose.
Patients retained on extended-release buprenorphine had fewer risk factors.
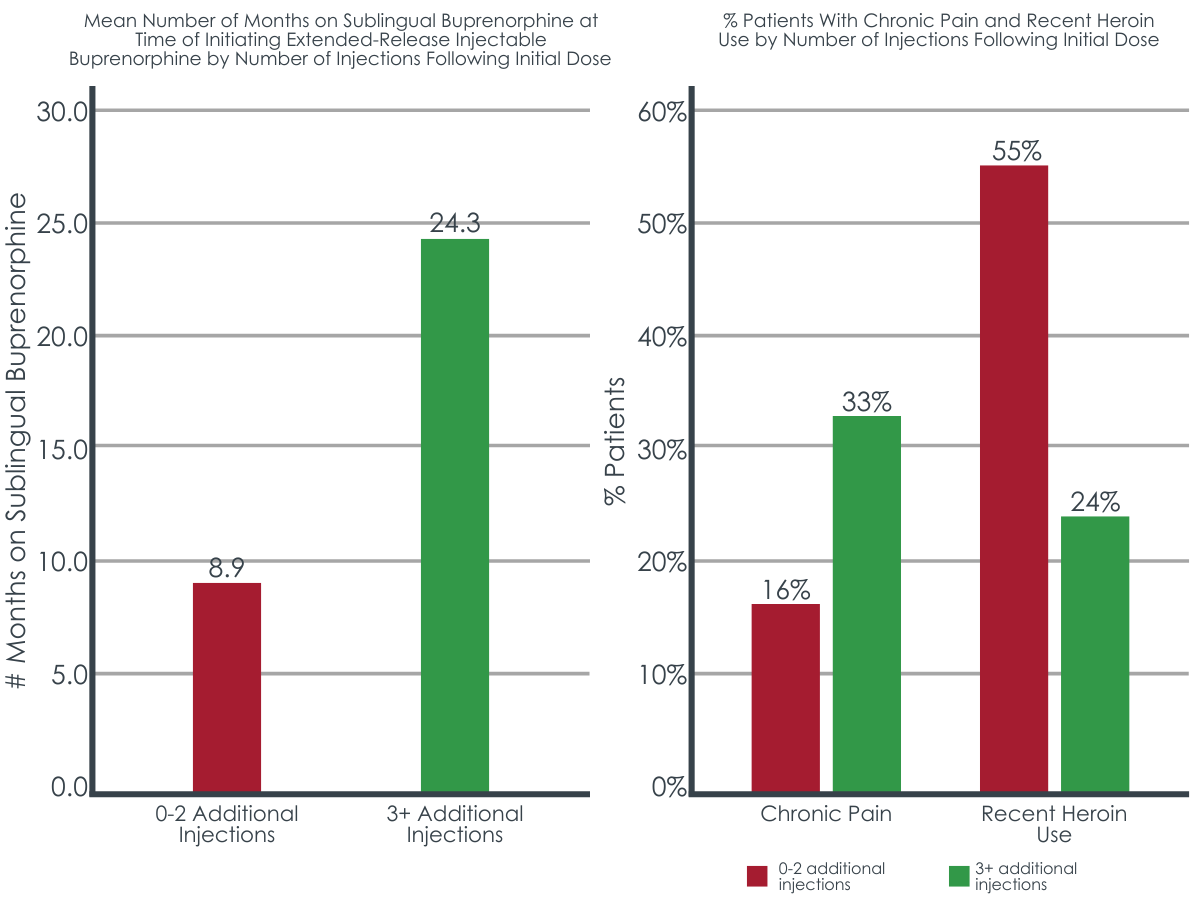
Patients who received three or more follow-up injections were on sublingual buprenorphine for about 15 months longer than those who received fewer than three injections (Mean duration: 24 months vs. 9 months). Chronic pain was more prevalent (33% vs. 16%) and heroin use in the three months prior to the first injection was less prevalent (24% vs. 55%) among those with three or more follow-up injections, compared to those with zero, one, or two injections of extended-release buprenorphine. While not quite reaching statistical significance, they appeared somewhat less likely to have a co-occurring mental health diagnosis (60% vs. 75%).
Most patients who discontinued extended-release injectable buprenorphine returned to sublingual buprenorphine treatment.
Of the patients who received fewer than 3 buprenorphine injections, 77% had returned to the sublingual formulation of buprenorphine within 45 days of their final injection, 7% discontinued altogether due to loss of insurance coverage, and 16% discontinued altogether for unknown reasons.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Retention is an ongoing issue for buprenorphine treatment, with a large majority of patients dropping out of treatment before the full benefits of pharmacotherapy are seen. This is particularly important in the context of buprenorphine because fewer than six months of treatment is associated with a significantly increased risk for opioid overdose and hospitalization. Despite extended-release injectable buprenorphine being a theoretically more convenient option than sublingual buprenorphine (e.g., monthly vs. daily dosing, fewer visits to the doctor, etc.), this study suggests that retention in treatment upon a transition to extended-release formulations of buprenorphine may also present difficulties. This seems particularly true for individuals with fewer months of prior buprenorphine treatment overall – people, arguably, who need it the most. However, it is important to note that most of the participants in this study were already receiving longer-term treatment with sublingual buprenorphine, with average treatment durations that were well beyond 6 months. Therefore, this represents a relatively stable group of patients who appear to be motivated in continuing medication use, as demonstrated by the high percentage of individuals who returned to sublingual buprenorphine when they stopped the injectable buprenorphine.
Despite most patients remaining on buprenorphine treatment in any formulation (sublingual or injectable), about one-quarter of the patients completely discontinued treatment within six months of attempting their transition to the extended-release formulation. Thus, transitioning to extended-release buprenorphine could potentially pose a risk to treatment continuity in certain patients established on sublingual formulations. Indeed, injection site reactions are just one factor that might deter individuals from long-term extended-release injectable buprenorphine treatment. Additionally, this study found that insurance coverage was a factor in discontinuation, emphasizing the need to ensure insurance coverage exists and can be maintained before deciding to transition a patient to the more costly extended-release versions of buprenorphine. Additional research is needed to determine the reasons underlying discontinuation in patients undergoing such transitions to better interpret treatment cessation as a positive or negative outcome in this context. Moreover, although about half of the individuals in this study received four or more total injections of extended-release buprenorphine, these may not have necessarily been consecutive monthly doses, as intended. Additional research looking at consistent monthly compliance with extended-release buprenorphine and the reasons for non-compliance are also needed.
This study also suggests that patients with chronic pain and without recent heroin use may be good candidates for transitioning to extended-release injectable buprenorphine, as a higher percentage of patients with these characteristics were retained in treatment relative to those who lacked these characteristics. Buprenorphine is sometimes used as a treatment for chronic pain and has previously been shown to reduce risk of buprenorphine treatment drop out in the first six months of opioid use disorder treatment. It may be that chronic pain comorbidities may help to enhance retention when patients are faced with a transition to a different buprenorphine formulation, as suggested in this study. Findings concerning heroin use are consistent with previous studies showing that recent heroin use is a predictor of lower retention in buprenorphine treatment, including treatment with extended-release formulations. Recent heroin use may be a sign of greater instability, even among these participants with relatively longer buprenorphine treatment durations, and such patients who returned to sublingual buprenorphine might prefer and benefit more greatly from daily dosing and more frequent check-ups with their doctors to enhance accountability. Additional research is needed to identify the reasons underlying discontinuation and to better understand patient outcomes after leaving treatment.
Importantly, this study did not include a comparison group that continued on sublingual buprenorphine, limiting conclusions around whether retention differs between those who continue sublingual and those who transition to extended-release injectable buprenorphine in real-world treatment settings.
The study sample was relatively small (n=92) and additional research with larger samples will better inform the accuracy and broader applicability of these findings. All patients had insurance that fully covered treatment with injectable extended-release buprenorphine and retention rates could differ for those with partial or no coverage given the greater financial burden of treatment.
This study did not include a comparison group of individuals who remained on sublingual buprenorphine, and it is therefore unclear if retention rates differ by buprenorphine formulation. The researchers did not report on the use of substances other than opioids, which limits interpretation given that other substance use is associated with worse retention in medication treatment.
Retention was defined as receiving 3 injections after the initial dose and additional research is needed to examine continuous retention in extended-release buprenorphine treatment through 6 months and beyond.
BOTTOM LINE
Despite extended-release once per month injectable buprenorphine being a theoretically more convenient option than taking buprenorphine daily (e.g., monthly vs. daily dosing, fewer visits to the doctor, etc.), this study suggests that obstacles may also exist for patients who transition to an extended-release formulation, especially among those who are in their first year of treatment. The majority of individuals who discontinued extended-release injectable buprenorphine returned to sublingual buprenorphine upon discontinuation but there is a subset of individuals who appear to be at risk of discontinuing pharmacotherapy altogether when transitioning to a new formulation. Additional research will help clarify the reasons for discontinuation and whether it is an unintended consequence or an intentional goal upon transition. Further investigation is important because extended-release buprenorphine has many potential benefits to patients (e.g., convenient once-monthly dosing for increasing compliance, reducing stigma, and allowing individuals to lead normal lives; houseless individuals not having to worry about medication storage to avoid theft, etc.).
For individuals and families seeking recovery: Buprenorphine is a helpful treatment for opioid use disorder that save lives. It comes in various formulations, including sublingual and extended-release injectable versions. Individuals who are doing well on sublingual buprenorphine and are looking to transition to a more convenient formulation, such as extended-release injectable buprenorphine, that does not require daily dosing should speak with their doctor about the risks and benefits of doing so. Individuals who are still struggling with ongoing illicit opioid use may benefit from staying on sublingual buprenorphine to ensure regular check-ups and more attentive care needed to better support treatment and recovery.
For treatment professionals and treatment systems: Given the potential variability of success in transitioning a patient from sublingual buprenorphine to extended-release injectable buprenorphine, treatment providers should be cautious with decisions to transition patients. Discussions around convenience, possible differences in side effects, insurance coverage, and patients’ treatment goals, as well as frequent evaluation of craving/withdrawal symptoms and patient well-being during transitions to different formulations are encouraged to support patients and enhance their engagement and retention in treatment. Individuals who have recently engaging in illicit opioid use may have a more difficult time with such transitions.
For scientists: Additional research is needed to examine retention upon a transition from sublingual buprenorphine to extended-release formulations, including the time at which the transition is made and the patient characteristics influencing successful transitions that enhance retention. Investigations in real-world populations within various settings (office-based primary-care settings vs. outpatient treatment programs) will help inform best practices. Studies implementing control groups for comparison (sublingual buprenorphine without transition to extended-release) and evaluating other forms of extended-release buprenorphine (e.g., implant) with long-term follow up and qualitative assessments for reasons underlying discontinuation are also needed.
For policy makers: Though opioid agonist medications (buprenorphine and methadone) are helpful life-saving medications for the treatment of opioid use disorder, retention in treatment is an ongoing issue that partially contributes to opioid overdose rates. Additional research funding will help identify best practice recommendations to maximize patient outcomes and reduce clinical and public health burdens of opioid use disorder. Examining patient characteristics that influence the uptake and impact of various pharmacotherapies will also inform new patient-centered approaches that better equip doctors to retain patients in treatment to promote successful remission and stable recovery.
Buprenorphine is a helpful medication for opioid use disorder, reducing opioid craving, misuse, and overdose risk. Sublingual buprenorphine was approved for opioid use disorder treatment in the United States in 2002 and is now the most commonly prescribed pharmacotherapy for the disorder. Because this form of the medication is taken daily and prescribed in office-based settings, there are concerns around medication adherence and treatment retention. About two-thirds of individuals stop taking their medication within six months of treatment, which increases risk of returning to illicit opioid use and overdosing. The need to dose daily and attend frequent office-based doctor visits to renew sublingual buprenorphine prescriptions might contribute to adherence and retention issues. Thus, long-acting injectable extended-release versions of the medication might help. Long-acting versions of another FDA approved medication in the treatment of opioid use disorder – long-acting naltrexone (sold under the brand Vivitrol) has shown helpful in increasing abstinence from illicit opioids and such long-acting variants of these medications may be particularly helpful for certain groups of people, such as those experiencing homelessness, who have been shown to have better outcomes on the extended release formulation of naltrexone (Vivitrol), compared to daily buprenorphine.
An extended-release injectable formulation of buprenorphine was approved in 2017 and is as safe and effective as sublingual formulations. This once monthly injectable requires fewer office visits and helps to prevent compliance issues seen with daily dosing. However, few studies have examined real-world treatment retention with injectable extended-release buprenorphine or patient characteristics that might influence it. Even fewer studies have evaluated retention among those who are transitioning to extended-release buprenorphine after longer-term daily dosed buprenorphine. Research on extended-release injectable buprenorphine can help improve opioid use disorder treatment recommendations. The current study examined real-world retention rates in patients transitioning from longer-term daily dosing to the injectable version, as well as factors that predict successful retention after transitioning.
HOW WAS THIS STUDY CONDUCTED?
The study examined electronic medical records to estimate 6-month retention on injectable extended-release buprenorphine in 92 consecutive patients with opioid use disorder who transitioned from sublingual (i.e., often prescribed in formulation with naloxone known by the brand name Suboxone) to injectable buprenorphine (i.e. of which Sublocade is one brand name formulation).
All participants were patients from a single treatment facility in Massachusetts who were stabilized on sublingual buprenorphine (8-24 mg per day) and had insurance that covered reimbursement for extended-release buprenorphine treatment.
Patients had been on sublingual buprenorphine for an average of 17 months and received their first extended-release buprenorphine injection between 2018 and 2019. In general, the first two injections (months 1 and 2) were 300 mg doses and subsequent injections (month 3 and later) were 100 mg doses. However, patients who experienced withdrawal or craving were supplemented with low doses (2-4 mg per day) of sublingual buprenorphine during the first two months of extended-release injectable buprenorphine treatment, and those who continued to experience withdrawal or craving at month 3 and beyond continued to receive 300 mg injections (instead of reducing to 100 mg).
Retention rate was examined as the proportion of individuals who received 0, 1, 2, and 3 or more follow-up injections within six months of their initial injection. Demographics, substance use history, and treatment history were also obtained from the medical records and the researchers examined whether these variables differed between patients who received 3 or more follow-up injections – the marker of “successful” retention in the current study – relative to those who received less than 3 doses.
The majority of participants were white (90%) men (67%) in their late thirties (average age of 38 years) with a history of injection drug use (73%). About 40% used heroin in the three months prior to their first buprenorphine injection. In terms of other current diagnoses, 34% had a chronic pain diagnosis and 67% had a comorbid psychiatric disorder (e.g., major depression, bipolar disorder, anxiety disorder, psychotic disorder).
WHAT DID THIS STUDY FIND?
About half of the patients were successfully retained on extended-release injectable buprenorphine.
Fifty-two percent of patients received three or more extended-release buprenorphine injections after their initial injection. Thirty-six percent of patients received one or two follow-up doses and 12% discontinued treatment after the first dose.
Patients retained on extended-release buprenorphine had fewer risk factors.
Patients who received three or more follow-up injections were on sublingual buprenorphine for about 15 months longer than those who received fewer than three injections (Mean duration: 24 months vs. 9 months). Chronic pain was more prevalent (33% vs. 16%) and heroin use in the three months prior to the first injection was less prevalent (24% vs. 55%) among those with three or more follow-up injections, compared to those with zero, one, or two injections of extended-release buprenorphine. While not quite reaching statistical significance, they appeared somewhat less likely to have a co-occurring mental health diagnosis (60% vs. 75%).
Most patients who discontinued extended-release injectable buprenorphine returned to sublingual buprenorphine treatment.
Of the patients who received fewer than 3 buprenorphine injections, 77% had returned to the sublingual formulation of buprenorphine within 45 days of their final injection, 7% discontinued altogether due to loss of insurance coverage, and 16% discontinued altogether for unknown reasons.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Retention is an ongoing issue for buprenorphine treatment, with a large majority of patients dropping out of treatment before the full benefits of pharmacotherapy are seen. This is particularly important in the context of buprenorphine because fewer than six months of treatment is associated with a significantly increased risk for opioid overdose and hospitalization. Despite extended-release injectable buprenorphine being a theoretically more convenient option than sublingual buprenorphine (e.g., monthly vs. daily dosing, fewer visits to the doctor, etc.), this study suggests that retention in treatment upon a transition to extended-release formulations of buprenorphine may also present difficulties. This seems particularly true for individuals with fewer months of prior buprenorphine treatment overall – people, arguably, who need it the most. However, it is important to note that most of the participants in this study were already receiving longer-term treatment with sublingual buprenorphine, with average treatment durations that were well beyond 6 months. Therefore, this represents a relatively stable group of patients who appear to be motivated in continuing medication use, as demonstrated by the high percentage of individuals who returned to sublingual buprenorphine when they stopped the injectable buprenorphine.
Despite most patients remaining on buprenorphine treatment in any formulation (sublingual or injectable), about one-quarter of the patients completely discontinued treatment within six months of attempting their transition to the extended-release formulation. Thus, transitioning to extended-release buprenorphine could potentially pose a risk to treatment continuity in certain patients established on sublingual formulations. Indeed, injection site reactions are just one factor that might deter individuals from long-term extended-release injectable buprenorphine treatment. Additionally, this study found that insurance coverage was a factor in discontinuation, emphasizing the need to ensure insurance coverage exists and can be maintained before deciding to transition a patient to the more costly extended-release versions of buprenorphine. Additional research is needed to determine the reasons underlying discontinuation in patients undergoing such transitions to better interpret treatment cessation as a positive or negative outcome in this context. Moreover, although about half of the individuals in this study received four or more total injections of extended-release buprenorphine, these may not have necessarily been consecutive monthly doses, as intended. Additional research looking at consistent monthly compliance with extended-release buprenorphine and the reasons for non-compliance are also needed.
This study also suggests that patients with chronic pain and without recent heroin use may be good candidates for transitioning to extended-release injectable buprenorphine, as a higher percentage of patients with these characteristics were retained in treatment relative to those who lacked these characteristics. Buprenorphine is sometimes used as a treatment for chronic pain and has previously been shown to reduce risk of buprenorphine treatment drop out in the first six months of opioid use disorder treatment. It may be that chronic pain comorbidities may help to enhance retention when patients are faced with a transition to a different buprenorphine formulation, as suggested in this study. Findings concerning heroin use are consistent with previous studies showing that recent heroin use is a predictor of lower retention in buprenorphine treatment, including treatment with extended-release formulations. Recent heroin use may be a sign of greater instability, even among these participants with relatively longer buprenorphine treatment durations, and such patients who returned to sublingual buprenorphine might prefer and benefit more greatly from daily dosing and more frequent check-ups with their doctors to enhance accountability. Additional research is needed to identify the reasons underlying discontinuation and to better understand patient outcomes after leaving treatment.
Importantly, this study did not include a comparison group that continued on sublingual buprenorphine, limiting conclusions around whether retention differs between those who continue sublingual and those who transition to extended-release injectable buprenorphine in real-world treatment settings.
The study sample was relatively small (n=92) and additional research with larger samples will better inform the accuracy and broader applicability of these findings. All patients had insurance that fully covered treatment with injectable extended-release buprenorphine and retention rates could differ for those with partial or no coverage given the greater financial burden of treatment.
This study did not include a comparison group of individuals who remained on sublingual buprenorphine, and it is therefore unclear if retention rates differ by buprenorphine formulation. The researchers did not report on the use of substances other than opioids, which limits interpretation given that other substance use is associated with worse retention in medication treatment.
Retention was defined as receiving 3 injections after the initial dose and additional research is needed to examine continuous retention in extended-release buprenorphine treatment through 6 months and beyond.
BOTTOM LINE
Despite extended-release once per month injectable buprenorphine being a theoretically more convenient option than taking buprenorphine daily (e.g., monthly vs. daily dosing, fewer visits to the doctor, etc.), this study suggests that obstacles may also exist for patients who transition to an extended-release formulation, especially among those who are in their first year of treatment. The majority of individuals who discontinued extended-release injectable buprenorphine returned to sublingual buprenorphine upon discontinuation but there is a subset of individuals who appear to be at risk of discontinuing pharmacotherapy altogether when transitioning to a new formulation. Additional research will help clarify the reasons for discontinuation and whether it is an unintended consequence or an intentional goal upon transition. Further investigation is important because extended-release buprenorphine has many potential benefits to patients (e.g., convenient once-monthly dosing for increasing compliance, reducing stigma, and allowing individuals to lead normal lives; houseless individuals not having to worry about medication storage to avoid theft, etc.).
For individuals and families seeking recovery: Buprenorphine is a helpful treatment for opioid use disorder that save lives. It comes in various formulations, including sublingual and extended-release injectable versions. Individuals who are doing well on sublingual buprenorphine and are looking to transition to a more convenient formulation, such as extended-release injectable buprenorphine, that does not require daily dosing should speak with their doctor about the risks and benefits of doing so. Individuals who are still struggling with ongoing illicit opioid use may benefit from staying on sublingual buprenorphine to ensure regular check-ups and more attentive care needed to better support treatment and recovery.
For treatment professionals and treatment systems: Given the potential variability of success in transitioning a patient from sublingual buprenorphine to extended-release injectable buprenorphine, treatment providers should be cautious with decisions to transition patients. Discussions around convenience, possible differences in side effects, insurance coverage, and patients’ treatment goals, as well as frequent evaluation of craving/withdrawal symptoms and patient well-being during transitions to different formulations are encouraged to support patients and enhance their engagement and retention in treatment. Individuals who have recently engaging in illicit opioid use may have a more difficult time with such transitions.
For scientists: Additional research is needed to examine retention upon a transition from sublingual buprenorphine to extended-release formulations, including the time at which the transition is made and the patient characteristics influencing successful transitions that enhance retention. Investigations in real-world populations within various settings (office-based primary-care settings vs. outpatient treatment programs) will help inform best practices. Studies implementing control groups for comparison (sublingual buprenorphine without transition to extended-release) and evaluating other forms of extended-release buprenorphine (e.g., implant) with long-term follow up and qualitative assessments for reasons underlying discontinuation are also needed.
For policy makers: Though opioid agonist medications (buprenorphine and methadone) are helpful life-saving medications for the treatment of opioid use disorder, retention in treatment is an ongoing issue that partially contributes to opioid overdose rates. Additional research funding will help identify best practice recommendations to maximize patient outcomes and reduce clinical and public health burdens of opioid use disorder. Examining patient characteristics that influence the uptake and impact of various pharmacotherapies will also inform new patient-centered approaches that better equip doctors to retain patients in treatment to promote successful remission and stable recovery.
Buprenorphine is a helpful medication for opioid use disorder, reducing opioid craving, misuse, and overdose risk. Sublingual buprenorphine was approved for opioid use disorder treatment in the United States in 2002 and is now the most commonly prescribed pharmacotherapy for the disorder. Because this form of the medication is taken daily and prescribed in office-based settings, there are concerns around medication adherence and treatment retention. About two-thirds of individuals stop taking their medication within six months of treatment, which increases risk of returning to illicit opioid use and overdosing. The need to dose daily and attend frequent office-based doctor visits to renew sublingual buprenorphine prescriptions might contribute to adherence and retention issues. Thus, long-acting injectable extended-release versions of the medication might help. Long-acting versions of another FDA approved medication in the treatment of opioid use disorder – long-acting naltrexone (sold under the brand Vivitrol) has shown helpful in increasing abstinence from illicit opioids and such long-acting variants of these medications may be particularly helpful for certain groups of people, such as those experiencing homelessness, who have been shown to have better outcomes on the extended release formulation of naltrexone (Vivitrol), compared to daily buprenorphine.
An extended-release injectable formulation of buprenorphine was approved in 2017 and is as safe and effective as sublingual formulations. This once monthly injectable requires fewer office visits and helps to prevent compliance issues seen with daily dosing. However, few studies have examined real-world treatment retention with injectable extended-release buprenorphine or patient characteristics that might influence it. Even fewer studies have evaluated retention among those who are transitioning to extended-release buprenorphine after longer-term daily dosed buprenorphine. Research on extended-release injectable buprenorphine can help improve opioid use disorder treatment recommendations. The current study examined real-world retention rates in patients transitioning from longer-term daily dosing to the injectable version, as well as factors that predict successful retention after transitioning.
HOW WAS THIS STUDY CONDUCTED?
The study examined electronic medical records to estimate 6-month retention on injectable extended-release buprenorphine in 92 consecutive patients with opioid use disorder who transitioned from sublingual (i.e., often prescribed in formulation with naloxone known by the brand name Suboxone) to injectable buprenorphine (i.e. of which Sublocade is one brand name formulation).
All participants were patients from a single treatment facility in Massachusetts who were stabilized on sublingual buprenorphine (8-24 mg per day) and had insurance that covered reimbursement for extended-release buprenorphine treatment.
Patients had been on sublingual buprenorphine for an average of 17 months and received their first extended-release buprenorphine injection between 2018 and 2019. In general, the first two injections (months 1 and 2) were 300 mg doses and subsequent injections (month 3 and later) were 100 mg doses. However, patients who experienced withdrawal or craving were supplemented with low doses (2-4 mg per day) of sublingual buprenorphine during the first two months of extended-release injectable buprenorphine treatment, and those who continued to experience withdrawal or craving at month 3 and beyond continued to receive 300 mg injections (instead of reducing to 100 mg).
Retention rate was examined as the proportion of individuals who received 0, 1, 2, and 3 or more follow-up injections within six months of their initial injection. Demographics, substance use history, and treatment history were also obtained from the medical records and the researchers examined whether these variables differed between patients who received 3 or more follow-up injections – the marker of “successful” retention in the current study – relative to those who received less than 3 doses.
The majority of participants were white (90%) men (67%) in their late thirties (average age of 38 years) with a history of injection drug use (73%). About 40% used heroin in the three months prior to their first buprenorphine injection. In terms of other current diagnoses, 34% had a chronic pain diagnosis and 67% had a comorbid psychiatric disorder (e.g., major depression, bipolar disorder, anxiety disorder, psychotic disorder).
WHAT DID THIS STUDY FIND?
About half of the patients were successfully retained on extended-release injectable buprenorphine.
Fifty-two percent of patients received three or more extended-release buprenorphine injections after their initial injection. Thirty-six percent of patients received one or two follow-up doses and 12% discontinued treatment after the first dose.
Patients retained on extended-release buprenorphine had fewer risk factors.
Patients who received three or more follow-up injections were on sublingual buprenorphine for about 15 months longer than those who received fewer than three injections (Mean duration: 24 months vs. 9 months). Chronic pain was more prevalent (33% vs. 16%) and heroin use in the three months prior to the first injection was less prevalent (24% vs. 55%) among those with three or more follow-up injections, compared to those with zero, one, or two injections of extended-release buprenorphine. While not quite reaching statistical significance, they appeared somewhat less likely to have a co-occurring mental health diagnosis (60% vs. 75%).
Most patients who discontinued extended-release injectable buprenorphine returned to sublingual buprenorphine treatment.
Of the patients who received fewer than 3 buprenorphine injections, 77% had returned to the sublingual formulation of buprenorphine within 45 days of their final injection, 7% discontinued altogether due to loss of insurance coverage, and 16% discontinued altogether for unknown reasons.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
Retention is an ongoing issue for buprenorphine treatment, with a large majority of patients dropping out of treatment before the full benefits of pharmacotherapy are seen. This is particularly important in the context of buprenorphine because fewer than six months of treatment is associated with a significantly increased risk for opioid overdose and hospitalization. Despite extended-release injectable buprenorphine being a theoretically more convenient option than sublingual buprenorphine (e.g., monthly vs. daily dosing, fewer visits to the doctor, etc.), this study suggests that retention in treatment upon a transition to extended-release formulations of buprenorphine may also present difficulties. This seems particularly true for individuals with fewer months of prior buprenorphine treatment overall – people, arguably, who need it the most. However, it is important to note that most of the participants in this study were already receiving longer-term treatment with sublingual buprenorphine, with average treatment durations that were well beyond 6 months. Therefore, this represents a relatively stable group of patients who appear to be motivated in continuing medication use, as demonstrated by the high percentage of individuals who returned to sublingual buprenorphine when they stopped the injectable buprenorphine.
Despite most patients remaining on buprenorphine treatment in any formulation (sublingual or injectable), about one-quarter of the patients completely discontinued treatment within six months of attempting their transition to the extended-release formulation. Thus, transitioning to extended-release buprenorphine could potentially pose a risk to treatment continuity in certain patients established on sublingual formulations. Indeed, injection site reactions are just one factor that might deter individuals from long-term extended-release injectable buprenorphine treatment. Additionally, this study found that insurance coverage was a factor in discontinuation, emphasizing the need to ensure insurance coverage exists and can be maintained before deciding to transition a patient to the more costly extended-release versions of buprenorphine. Additional research is needed to determine the reasons underlying discontinuation in patients undergoing such transitions to better interpret treatment cessation as a positive or negative outcome in this context. Moreover, although about half of the individuals in this study received four or more total injections of extended-release buprenorphine, these may not have necessarily been consecutive monthly doses, as intended. Additional research looking at consistent monthly compliance with extended-release buprenorphine and the reasons for non-compliance are also needed.
This study also suggests that patients with chronic pain and without recent heroin use may be good candidates for transitioning to extended-release injectable buprenorphine, as a higher percentage of patients with these characteristics were retained in treatment relative to those who lacked these characteristics. Buprenorphine is sometimes used as a treatment for chronic pain and has previously been shown to reduce risk of buprenorphine treatment drop out in the first six months of opioid use disorder treatment. It may be that chronic pain comorbidities may help to enhance retention when patients are faced with a transition to a different buprenorphine formulation, as suggested in this study. Findings concerning heroin use are consistent with previous studies showing that recent heroin use is a predictor of lower retention in buprenorphine treatment, including treatment with extended-release formulations. Recent heroin use may be a sign of greater instability, even among these participants with relatively longer buprenorphine treatment durations, and such patients who returned to sublingual buprenorphine might prefer and benefit more greatly from daily dosing and more frequent check-ups with their doctors to enhance accountability. Additional research is needed to identify the reasons underlying discontinuation and to better understand patient outcomes after leaving treatment.
Importantly, this study did not include a comparison group that continued on sublingual buprenorphine, limiting conclusions around whether retention differs between those who continue sublingual and those who transition to extended-release injectable buprenorphine in real-world treatment settings.
The study sample was relatively small (n=92) and additional research with larger samples will better inform the accuracy and broader applicability of these findings. All patients had insurance that fully covered treatment with injectable extended-release buprenorphine and retention rates could differ for those with partial or no coverage given the greater financial burden of treatment.
This study did not include a comparison group of individuals who remained on sublingual buprenorphine, and it is therefore unclear if retention rates differ by buprenorphine formulation. The researchers did not report on the use of substances other than opioids, which limits interpretation given that other substance use is associated with worse retention in medication treatment.
Retention was defined as receiving 3 injections after the initial dose and additional research is needed to examine continuous retention in extended-release buprenorphine treatment through 6 months and beyond.
BOTTOM LINE
Despite extended-release once per month injectable buprenorphine being a theoretically more convenient option than taking buprenorphine daily (e.g., monthly vs. daily dosing, fewer visits to the doctor, etc.), this study suggests that obstacles may also exist for patients who transition to an extended-release formulation, especially among those who are in their first year of treatment. The majority of individuals who discontinued extended-release injectable buprenorphine returned to sublingual buprenorphine upon discontinuation but there is a subset of individuals who appear to be at risk of discontinuing pharmacotherapy altogether when transitioning to a new formulation. Additional research will help clarify the reasons for discontinuation and whether it is an unintended consequence or an intentional goal upon transition. Further investigation is important because extended-release buprenorphine has many potential benefits to patients (e.g., convenient once-monthly dosing for increasing compliance, reducing stigma, and allowing individuals to lead normal lives; houseless individuals not having to worry about medication storage to avoid theft, etc.).
For individuals and families seeking recovery: Buprenorphine is a helpful treatment for opioid use disorder that save lives. It comes in various formulations, including sublingual and extended-release injectable versions. Individuals who are doing well on sublingual buprenorphine and are looking to transition to a more convenient formulation, such as extended-release injectable buprenorphine, that does not require daily dosing should speak with their doctor about the risks and benefits of doing so. Individuals who are still struggling with ongoing illicit opioid use may benefit from staying on sublingual buprenorphine to ensure regular check-ups and more attentive care needed to better support treatment and recovery.
For treatment professionals and treatment systems: Given the potential variability of success in transitioning a patient from sublingual buprenorphine to extended-release injectable buprenorphine, treatment providers should be cautious with decisions to transition patients. Discussions around convenience, possible differences in side effects, insurance coverage, and patients’ treatment goals, as well as frequent evaluation of craving/withdrawal symptoms and patient well-being during transitions to different formulations are encouraged to support patients and enhance their engagement and retention in treatment. Individuals who have recently engaging in illicit opioid use may have a more difficult time with such transitions.
For scientists: Additional research is needed to examine retention upon a transition from sublingual buprenorphine to extended-release formulations, including the time at which the transition is made and the patient characteristics influencing successful transitions that enhance retention. Investigations in real-world populations within various settings (office-based primary-care settings vs. outpatient treatment programs) will help inform best practices. Studies implementing control groups for comparison (sublingual buprenorphine without transition to extended-release) and evaluating other forms of extended-release buprenorphine (e.g., implant) with long-term follow up and qualitative assessments for reasons underlying discontinuation are also needed.
For policy makers: Though opioid agonist medications (buprenorphine and methadone) are helpful life-saving medications for the treatment of opioid use disorder, retention in treatment is an ongoing issue that partially contributes to opioid overdose rates. Additional research funding will help identify best practice recommendations to maximize patient outcomes and reduce clinical and public health burdens of opioid use disorder. Examining patient characteristics that influence the uptake and impact of various pharmacotherapies will also inform new patient-centered approaches that better equip doctors to retain patients in treatment to promote successful remission and stable recovery.