What is promised versus what gets delivered in LGBTQ addiction care
LGBTQ individuals as a population have higher rates of non-medical prescription opioid use and opioid use disorderrelative to the general population. This study characterized how available programs might be that address the unique needs of LGBTQ individuals with opioid use disorder.
Additionally, some LGBTQ community members may avoid seeking care because they anticipate experiencing discrimination from their providers. Utilization of LGBTQ-specific treatment for opioid use disorder could help close the gap in treatment in the LGBTQ community. To date, however, it is unclear to what degree such treatment is available and accessible for these individuals. The present study simulated the experience of searching for LGBTQ-specific opioid use disorder treatment to demonstrate the practical availability of such care in the US.
HOW WAS THIS STUDY CONDUCTED?
This was a descriptive study in which the research team contacted programs from the SAMHSA 2018 Treatment Directory which listed both medication for opioid use disorder services and LGBTQ-specific programs. The primary goal was to demonstrate the real-world availability LGBTQ-specific opioid use disorder treatments in the US. To this end, descriptive statistics were used to characterize the outcome of inquiries into services offered at treatment facilities across the US. The study also examined the degree to which such services were available in the 20 states with the highest rates of opioid-relate overdose (in the entire population irrespective of LGBTQ status).
The authors searched the SAMHSA Treatment Directory for facilities that listed themselves as providing both medication for opioid use disorder services and “special programs/groups” for LGBTQ clients. To identify eligible treatment facilities, the authors included sites that listed offering 1) “Substance Use (SU)” services and “Substance Use Treatment” under “Type of Care” and 2) “Lesbian, gay, bisexual, or transgender clients” under “Special Programs/Groups Offered”. Results were then downloaded into a Microsoft Excel file. The list was further culled by excluding facilities that did not indicate offering medications for opioid use disorder. Finally, the authors restricted the list of facilities to those in the top 20 states with the highest national opioid overdose rates (according to data available at the time of the study). These states were: Connecticut, Illinois, Kentucky, Massachusetts, Maryland, Maine, Michigan, Missouri, North Carolina, New Hampshire, New Mexico, New York, Ohio, Rhode Island, South Carolina, Tennessee, Vermont, Wisconsin, West Virginia, and Washington, D.C.
Research assistants contacted each facility to determine the correspondence between services listed on the Directory and those offered onsite. Research Assistants called facilities during regular business hours and used an identical script to ask the staff member for information about the advertised services and recorded their responses. Scripted questions included “Hi, I found the listing for your agency in the SAMHSA Treatment Services Locator, and it says that you offer special programs and groups for LGBT people, so I was wondering if I could get some more information about that?” and “Your Directory listing also mentions that you offer medication-assisted treatment for opioid use disorders. Can you tell me what types of [medications for opioid use disorder] you offer?” Due to the COVID-19 pandemic, additional responses were added to the script- if facility staff indicated they had discontinued/adjusted services due to COVID-19, the research assistant stated, “I understand, but could you tell me about the services that you usually offer or were offering before this happened?” Research assistants did not ask staff members to disclose any personal information, nor to engage in activities beyond providing information about available services. Each facility was contacted up to 3 times before being deemed unreachable.
All facilities were contacted between January 17, 2020 and October 15, 2020. A total of 570 treatment facilities listed themselves as providing both medication for opioid use disorder and 2) “special programs/groups” for LGBTQ clients. Of these facilities, the authors successfully contacted 446 (78.5%). Reasons for unsuccessful contact of the remaining 124 facilities included: no answer (31.5%); the research assistant being transferred multiple times without reaching someone who could answer their questions (25.0%); being unable to reach a live person (23.4%); the information being unavailable due to COVID-19 disruptions (e.g., operator stating that the facility was not answering calls due to the pandemic; 12.1%); and the listed phone number being incorrect (8.1%).
WHAT DID THIS STUDY FIND?
Staff outreach confirmed most of the facilities listed as offering medications for opioid use disorders
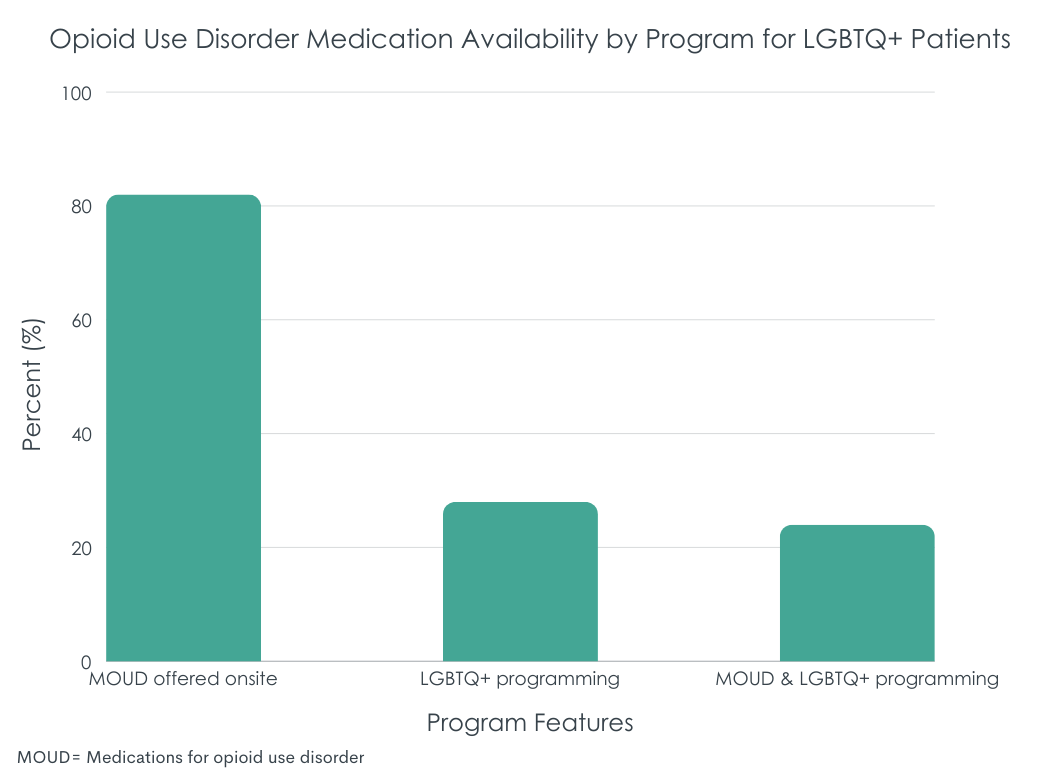
Of the 446 facilities reached, 82.1% (366) reported offering medications for opioid use disorder consistent with the information listed in the SAMHSA Treatment Directory. Medications offered included buprenorphine in formulation with naloxone also known by the brand name Suboxone (n=271, 74.0%), buprenorphine formulations apart from commonly prescribed Suboxone (n=182, 49.7%), methadone (n=145, 39.6%), extended-release injectable naltrexone also known by the brand name Vivitrol (n=142, 38.8%), and extended-release injectable buprenorphine, also known by the brand name Sublocade (n=14, 3.8%).
Staff outreach did not confirm most facilities listed as offering LGBTQ-specific services
Less than 30% (n=125) of 446 of facilities reached confirmed that they offered special programs or groups for LGBTQ clients despite listing those services in the SAMHSA Treatment Directory. These services included LGBTQ-friendly counseling (n=82, 65.6%) and LGBTQ-specific support groups (n=12, 9.6%). Less than a quarter of facilities (n=107) that were listed in the directory as offering both medications for opioid use disorder and LGBTQ-specific treatment were confirmed as offering both services.
The availability of LGBTQ-specific services and medications for opioid use disorder varied by state
Among the 20 states with the highest rates of opioid-related overdose, less than 80% (n=43) of facilities in each of Missouri, New Mexico, Connecticut, and Illinois reported offering medications for opioid use disorder – which tended to be lower than other states. Over 30% (n=72) of facilitates in each of Michigan, New York, Massachusetts, and Missouri reported offering LGBTQ-specific services – which tended to be higher than most other states. Only New York, Massachusetts, and Missouri had more than 30% offering both medications for opioid use disorder and LGBTQ-specific services (n=58).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that programs offering both opioid use disorder medications and tailored programming for the LGBTQ community are not widely available in many parts of the US. Although all the treatment facilities contacted by the authors had self-reported to SAMHSA that they offered both medications for opioid use disorder and LGBTQ-specific services, facility staff confirmed this was not the case for most treatment centers. The authors also found that the availability of these services varied regionally with states in the Northeastern US (New York and Massachusetts) having the highest availability of these services. Of note, however, over 30% of facilities contacted in Missouri also offered these services.
Taken together, these results may indicate that a noteworthy dearth of opioid use disorder services available to the LGBTQ community. This research builds upon previous work demonstrating discrepancies in theavailability of LGBTQ-specific treatment in the US. The fact that the availability of such services is so limited is concerning. LGBTQ-specific treatment programs are known to foster positive treatment outcomes for LGBTQ clients. The limited availability of such services represents a barrier to LGBTQ individuals from receiving effective care. That is, lower availability of LGBTQ-specific approaches in substance use disorder treatment settings may be a barrier to engaging with care. It is unclear exactly why such services are not widely available. One reason may be the absence of evidence-based protocols specifically for LGBTQ individuals with opioid use disorder. Future work is needed to understand what barriers facilities may encounter to implement inclusive care (e.g., operation costs, any contextual effects of low local LGBTQ population density, difficulty accessing evidence-based care designed for this group, etc.).
The current research cannot answer why discrepancies between listed and offered LGBTQ-specific services exist. It is possible that in some cases LGBTQ-specific programs may have been discontinued during the time between when representatives for the facilities reported their services to SAMHSA and when the facilities were contacted. This is somewhat supported in the article – the authors note that 4.3% of contacted facilities said that they had discontinued their LGBTQ-specific groups due to the COVID-19 pandemic. This does not account for the wide discrepancy between listed and offered services but does suggest that some treatment centers may have been forced to stop offering services due to extenuating circumstances. It is also possible that some of these facilities may have been attempting to market to a wider audience (i.e., the LGBTQ community). Regardless, the current study suggests that the way treatment facilities report what services they offer to SAMHSA would benefit from a closer look. A verification process, for example, may increase accuracy – which is important to understand treatment access facilitators and barriers for vulnerable groups like the LGBTQ community.
Unlike similar researchconducted previously, the current research did not examine availability of LGBTQ-specific opioid use disorder treatment across the entire US. Because the authors limited facilities to states with the top 20 highest opioid overdose rates, they may have missed valuable data from other states.
The study did not account for local LGBTQ-population density when assessing availability. That is, it seems possible that in some areas (particularly low population rural regions) the number of LGBTQ-identified people may be lower than states with more urban centers. As such, there likely would be less demand for specialized substance use disorder in such areas. It may have been more helpful for the authors to have employed some sort of weighting techniques to demonstrate availability of LGBTQ-specific services proportional to endemic LGBTQ populations.
BOTTOM LINE
This study found that there were discrepancies between the services listed on a national registry of substance use disorder treatment facilities and the available services at those facilities. Specifically, only ~24% of treatment facilities which reported to SAMHSA that they provided both medications for opioid use disorder and LGBTQ-specific reported that they had both types of these services when contacted directly. The authors also found that these discrepancies varied across states. Facilities in New York, Massachusetts, and Missouri had the highest congruence between listed and offered services. This study adds to the literature showing limited availability of opioid use disorder treatment specific to the needs of LGBTQ populations in the US. Expansion of such services are critical as they would be a vital tool in addressing LGBTQ opioid-related health disparities. It is critical for more research to be conducted demonstrating why medications for opioid use disorder and LGBT-specific services may not be more widely available.
For individuals and families seeking recovery: It may be challenging to find opioid use disorder treatment tailored to meet the needs of LGBTQ individuals. Importantly this study showed that even when treatment facilities list that they do offer such care – this may not be the case in practice. This suggests that those seeking recovery services for themselves or others need to be especially diligent in searching for services capable of meeting the unique needs of LGBTQ patients. For example, it may be more fruitful to research local providers to ensure they have experience working with the LGBT community and/or who have received special training in fields relevant for these populations (e.g., gender affirming care). Once potential programs or providers are identified, it could be beneficial to reach out to them directly to confirm they have the expertise needed to meet the needs of LGBTQ clients.
For treatment professionals and treatment systems: The present study suggests that LGBTQ individuals may encounter barriers to receiving effective opioid use disorder care. This is consistent with other similar work illustrating limited access to LGBTQ-specific substance use treatment in the US. It is critically important for providers to account for potential barriers members of the LGBTQ community face when accessing care (e.g., social stigma towards LGBTQ people). It would be useful for providers and their staff to assess their current care environment and determine how it may need to be modified to accommodate the needs of the LGBTQ community. This may include incorporating cultural humility practices into care.
For scientists: The field may benefit from research examining reasons why treatment facilities that offer medications for opioid use disorder do not also include LGBTQ-specific services. Determining what may be preventing these services from being implemented could help determine how to address barriers to LGBTQ-specific care implementation. For example, it is possible that implementing these programs may be too burdensome for smaller facilities with limited funding.
For policy makers: Policy makers may consider implementing programs to address the needs of patients in substance use treatment who are also members of the LGBTQ community. One solution could be to reduce barriers to substance use treatment (e.g., through Medicaid expansion). Furthermore, it may be valuable to offer incentives to treatment providers to pursue training in LGBTQ-specific care. For example, the American Medical Association provides continuing education in LGBTQ-relevant issues to medical care providers. Analogous programs for substance use treatment providers which offer course credits could lead to increased availability of LGBTQ-specific substance use treatment. Trainings like these could also reduce anti-LGBTQ bias within substance use treatment contexts.
Additionally, some LGBTQ community members may avoid seeking care because they anticipate experiencing discrimination from their providers. Utilization of LGBTQ-specific treatment for opioid use disorder could help close the gap in treatment in the LGBTQ community. To date, however, it is unclear to what degree such treatment is available and accessible for these individuals. The present study simulated the experience of searching for LGBTQ-specific opioid use disorder treatment to demonstrate the practical availability of such care in the US.
HOW WAS THIS STUDY CONDUCTED?
This was a descriptive study in which the research team contacted programs from the SAMHSA 2018 Treatment Directory which listed both medication for opioid use disorder services and LGBTQ-specific programs. The primary goal was to demonstrate the real-world availability LGBTQ-specific opioid use disorder treatments in the US. To this end, descriptive statistics were used to characterize the outcome of inquiries into services offered at treatment facilities across the US. The study also examined the degree to which such services were available in the 20 states with the highest rates of opioid-relate overdose (in the entire population irrespective of LGBTQ status).
The authors searched the SAMHSA Treatment Directory for facilities that listed themselves as providing both medication for opioid use disorder services and “special programs/groups” for LGBTQ clients. To identify eligible treatment facilities, the authors included sites that listed offering 1) “Substance Use (SU)” services and “Substance Use Treatment” under “Type of Care” and 2) “Lesbian, gay, bisexual, or transgender clients” under “Special Programs/Groups Offered”. Results were then downloaded into a Microsoft Excel file. The list was further culled by excluding facilities that did not indicate offering medications for opioid use disorder. Finally, the authors restricted the list of facilities to those in the top 20 states with the highest national opioid overdose rates (according to data available at the time of the study). These states were: Connecticut, Illinois, Kentucky, Massachusetts, Maryland, Maine, Michigan, Missouri, North Carolina, New Hampshire, New Mexico, New York, Ohio, Rhode Island, South Carolina, Tennessee, Vermont, Wisconsin, West Virginia, and Washington, D.C.
Research assistants contacted each facility to determine the correspondence between services listed on the Directory and those offered onsite. Research Assistants called facilities during regular business hours and used an identical script to ask the staff member for information about the advertised services and recorded their responses. Scripted questions included “Hi, I found the listing for your agency in the SAMHSA Treatment Services Locator, and it says that you offer special programs and groups for LGBT people, so I was wondering if I could get some more information about that?” and “Your Directory listing also mentions that you offer medication-assisted treatment for opioid use disorders. Can you tell me what types of [medications for opioid use disorder] you offer?” Due to the COVID-19 pandemic, additional responses were added to the script- if facility staff indicated they had discontinued/adjusted services due to COVID-19, the research assistant stated, “I understand, but could you tell me about the services that you usually offer or were offering before this happened?” Research assistants did not ask staff members to disclose any personal information, nor to engage in activities beyond providing information about available services. Each facility was contacted up to 3 times before being deemed unreachable.
All facilities were contacted between January 17, 2020 and October 15, 2020. A total of 570 treatment facilities listed themselves as providing both medication for opioid use disorder and 2) “special programs/groups” for LGBTQ clients. Of these facilities, the authors successfully contacted 446 (78.5%). Reasons for unsuccessful contact of the remaining 124 facilities included: no answer (31.5%); the research assistant being transferred multiple times without reaching someone who could answer their questions (25.0%); being unable to reach a live person (23.4%); the information being unavailable due to COVID-19 disruptions (e.g., operator stating that the facility was not answering calls due to the pandemic; 12.1%); and the listed phone number being incorrect (8.1%).
WHAT DID THIS STUDY FIND?
Staff outreach confirmed most of the facilities listed as offering medications for opioid use disorders
Of the 446 facilities reached, 82.1% (366) reported offering medications for opioid use disorder consistent with the information listed in the SAMHSA Treatment Directory. Medications offered included buprenorphine in formulation with naloxone also known by the brand name Suboxone (n=271, 74.0%), buprenorphine formulations apart from commonly prescribed Suboxone (n=182, 49.7%), methadone (n=145, 39.6%), extended-release injectable naltrexone also known by the brand name Vivitrol (n=142, 38.8%), and extended-release injectable buprenorphine, also known by the brand name Sublocade (n=14, 3.8%).
Staff outreach did not confirm most facilities listed as offering LGBTQ-specific services
Less than 30% (n=125) of 446 of facilities reached confirmed that they offered special programs or groups for LGBTQ clients despite listing those services in the SAMHSA Treatment Directory. These services included LGBTQ-friendly counseling (n=82, 65.6%) and LGBTQ-specific support groups (n=12, 9.6%). Less than a quarter of facilities (n=107) that were listed in the directory as offering both medications for opioid use disorder and LGBTQ-specific treatment were confirmed as offering both services.
The availability of LGBTQ-specific services and medications for opioid use disorder varied by state
Among the 20 states with the highest rates of opioid-related overdose, less than 80% (n=43) of facilities in each of Missouri, New Mexico, Connecticut, and Illinois reported offering medications for opioid use disorder – which tended to be lower than other states. Over 30% (n=72) of facilitates in each of Michigan, New York, Massachusetts, and Missouri reported offering LGBTQ-specific services – which tended to be higher than most other states. Only New York, Massachusetts, and Missouri had more than 30% offering both medications for opioid use disorder and LGBTQ-specific services (n=58).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that programs offering both opioid use disorder medications and tailored programming for the LGBTQ community are not widely available in many parts of the US. Although all the treatment facilities contacted by the authors had self-reported to SAMHSA that they offered both medications for opioid use disorder and LGBTQ-specific services, facility staff confirmed this was not the case for most treatment centers. The authors also found that the availability of these services varied regionally with states in the Northeastern US (New York and Massachusetts) having the highest availability of these services. Of note, however, over 30% of facilities contacted in Missouri also offered these services.
Taken together, these results may indicate that a noteworthy dearth of opioid use disorder services available to the LGBTQ community. This research builds upon previous work demonstrating discrepancies in theavailability of LGBTQ-specific treatment in the US. The fact that the availability of such services is so limited is concerning. LGBTQ-specific treatment programs are known to foster positive treatment outcomes for LGBTQ clients. The limited availability of such services represents a barrier to LGBTQ individuals from receiving effective care. That is, lower availability of LGBTQ-specific approaches in substance use disorder treatment settings may be a barrier to engaging with care. It is unclear exactly why such services are not widely available. One reason may be the absence of evidence-based protocols specifically for LGBTQ individuals with opioid use disorder. Future work is needed to understand what barriers facilities may encounter to implement inclusive care (e.g., operation costs, any contextual effects of low local LGBTQ population density, difficulty accessing evidence-based care designed for this group, etc.).
The current research cannot answer why discrepancies between listed and offered LGBTQ-specific services exist. It is possible that in some cases LGBTQ-specific programs may have been discontinued during the time between when representatives for the facilities reported their services to SAMHSA and when the facilities were contacted. This is somewhat supported in the article – the authors note that 4.3% of contacted facilities said that they had discontinued their LGBTQ-specific groups due to the COVID-19 pandemic. This does not account for the wide discrepancy between listed and offered services but does suggest that some treatment centers may have been forced to stop offering services due to extenuating circumstances. It is also possible that some of these facilities may have been attempting to market to a wider audience (i.e., the LGBTQ community). Regardless, the current study suggests that the way treatment facilities report what services they offer to SAMHSA would benefit from a closer look. A verification process, for example, may increase accuracy – which is important to understand treatment access facilitators and barriers for vulnerable groups like the LGBTQ community.
Unlike similar researchconducted previously, the current research did not examine availability of LGBTQ-specific opioid use disorder treatment across the entire US. Because the authors limited facilities to states with the top 20 highest opioid overdose rates, they may have missed valuable data from other states.
The study did not account for local LGBTQ-population density when assessing availability. That is, it seems possible that in some areas (particularly low population rural regions) the number of LGBTQ-identified people may be lower than states with more urban centers. As such, there likely would be less demand for specialized substance use disorder in such areas. It may have been more helpful for the authors to have employed some sort of weighting techniques to demonstrate availability of LGBTQ-specific services proportional to endemic LGBTQ populations.
BOTTOM LINE
This study found that there were discrepancies between the services listed on a national registry of substance use disorder treatment facilities and the available services at those facilities. Specifically, only ~24% of treatment facilities which reported to SAMHSA that they provided both medications for opioid use disorder and LGBTQ-specific reported that they had both types of these services when contacted directly. The authors also found that these discrepancies varied across states. Facilities in New York, Massachusetts, and Missouri had the highest congruence between listed and offered services. This study adds to the literature showing limited availability of opioid use disorder treatment specific to the needs of LGBTQ populations in the US. Expansion of such services are critical as they would be a vital tool in addressing LGBTQ opioid-related health disparities. It is critical for more research to be conducted demonstrating why medications for opioid use disorder and LGBT-specific services may not be more widely available.
For individuals and families seeking recovery: It may be challenging to find opioid use disorder treatment tailored to meet the needs of LGBTQ individuals. Importantly this study showed that even when treatment facilities list that they do offer such care – this may not be the case in practice. This suggests that those seeking recovery services for themselves or others need to be especially diligent in searching for services capable of meeting the unique needs of LGBTQ patients. For example, it may be more fruitful to research local providers to ensure they have experience working with the LGBT community and/or who have received special training in fields relevant for these populations (e.g., gender affirming care). Once potential programs or providers are identified, it could be beneficial to reach out to them directly to confirm they have the expertise needed to meet the needs of LGBTQ clients.
For treatment professionals and treatment systems: The present study suggests that LGBTQ individuals may encounter barriers to receiving effective opioid use disorder care. This is consistent with other similar work illustrating limited access to LGBTQ-specific substance use treatment in the US. It is critically important for providers to account for potential barriers members of the LGBTQ community face when accessing care (e.g., social stigma towards LGBTQ people). It would be useful for providers and their staff to assess their current care environment and determine how it may need to be modified to accommodate the needs of the LGBTQ community. This may include incorporating cultural humility practices into care.
For scientists: The field may benefit from research examining reasons why treatment facilities that offer medications for opioid use disorder do not also include LGBTQ-specific services. Determining what may be preventing these services from being implemented could help determine how to address barriers to LGBTQ-specific care implementation. For example, it is possible that implementing these programs may be too burdensome for smaller facilities with limited funding.
For policy makers: Policy makers may consider implementing programs to address the needs of patients in substance use treatment who are also members of the LGBTQ community. One solution could be to reduce barriers to substance use treatment (e.g., through Medicaid expansion). Furthermore, it may be valuable to offer incentives to treatment providers to pursue training in LGBTQ-specific care. For example, the American Medical Association provides continuing education in LGBTQ-relevant issues to medical care providers. Analogous programs for substance use treatment providers which offer course credits could lead to increased availability of LGBTQ-specific substance use treatment. Trainings like these could also reduce anti-LGBTQ bias within substance use treatment contexts.
Additionally, some LGBTQ community members may avoid seeking care because they anticipate experiencing discrimination from their providers. Utilization of LGBTQ-specific treatment for opioid use disorder could help close the gap in treatment in the LGBTQ community. To date, however, it is unclear to what degree such treatment is available and accessible for these individuals. The present study simulated the experience of searching for LGBTQ-specific opioid use disorder treatment to demonstrate the practical availability of such care in the US.
HOW WAS THIS STUDY CONDUCTED?
This was a descriptive study in which the research team contacted programs from the SAMHSA 2018 Treatment Directory which listed both medication for opioid use disorder services and LGBTQ-specific programs. The primary goal was to demonstrate the real-world availability LGBTQ-specific opioid use disorder treatments in the US. To this end, descriptive statistics were used to characterize the outcome of inquiries into services offered at treatment facilities across the US. The study also examined the degree to which such services were available in the 20 states with the highest rates of opioid-relate overdose (in the entire population irrespective of LGBTQ status).
The authors searched the SAMHSA Treatment Directory for facilities that listed themselves as providing both medication for opioid use disorder services and “special programs/groups” for LGBTQ clients. To identify eligible treatment facilities, the authors included sites that listed offering 1) “Substance Use (SU)” services and “Substance Use Treatment” under “Type of Care” and 2) “Lesbian, gay, bisexual, or transgender clients” under “Special Programs/Groups Offered”. Results were then downloaded into a Microsoft Excel file. The list was further culled by excluding facilities that did not indicate offering medications for opioid use disorder. Finally, the authors restricted the list of facilities to those in the top 20 states with the highest national opioid overdose rates (according to data available at the time of the study). These states were: Connecticut, Illinois, Kentucky, Massachusetts, Maryland, Maine, Michigan, Missouri, North Carolina, New Hampshire, New Mexico, New York, Ohio, Rhode Island, South Carolina, Tennessee, Vermont, Wisconsin, West Virginia, and Washington, D.C.
Research assistants contacted each facility to determine the correspondence between services listed on the Directory and those offered onsite. Research Assistants called facilities during regular business hours and used an identical script to ask the staff member for information about the advertised services and recorded their responses. Scripted questions included “Hi, I found the listing for your agency in the SAMHSA Treatment Services Locator, and it says that you offer special programs and groups for LGBT people, so I was wondering if I could get some more information about that?” and “Your Directory listing also mentions that you offer medication-assisted treatment for opioid use disorders. Can you tell me what types of [medications for opioid use disorder] you offer?” Due to the COVID-19 pandemic, additional responses were added to the script- if facility staff indicated they had discontinued/adjusted services due to COVID-19, the research assistant stated, “I understand, but could you tell me about the services that you usually offer or were offering before this happened?” Research assistants did not ask staff members to disclose any personal information, nor to engage in activities beyond providing information about available services. Each facility was contacted up to 3 times before being deemed unreachable.
All facilities were contacted between January 17, 2020 and October 15, 2020. A total of 570 treatment facilities listed themselves as providing both medication for opioid use disorder and 2) “special programs/groups” for LGBTQ clients. Of these facilities, the authors successfully contacted 446 (78.5%). Reasons for unsuccessful contact of the remaining 124 facilities included: no answer (31.5%); the research assistant being transferred multiple times without reaching someone who could answer their questions (25.0%); being unable to reach a live person (23.4%); the information being unavailable due to COVID-19 disruptions (e.g., operator stating that the facility was not answering calls due to the pandemic; 12.1%); and the listed phone number being incorrect (8.1%).
WHAT DID THIS STUDY FIND?
Staff outreach confirmed most of the facilities listed as offering medications for opioid use disorders
Of the 446 facilities reached, 82.1% (366) reported offering medications for opioid use disorder consistent with the information listed in the SAMHSA Treatment Directory. Medications offered included buprenorphine in formulation with naloxone also known by the brand name Suboxone (n=271, 74.0%), buprenorphine formulations apart from commonly prescribed Suboxone (n=182, 49.7%), methadone (n=145, 39.6%), extended-release injectable naltrexone also known by the brand name Vivitrol (n=142, 38.8%), and extended-release injectable buprenorphine, also known by the brand name Sublocade (n=14, 3.8%).
Staff outreach did not confirm most facilities listed as offering LGBTQ-specific services
Less than 30% (n=125) of 446 of facilities reached confirmed that they offered special programs or groups for LGBTQ clients despite listing those services in the SAMHSA Treatment Directory. These services included LGBTQ-friendly counseling (n=82, 65.6%) and LGBTQ-specific support groups (n=12, 9.6%). Less than a quarter of facilities (n=107) that were listed in the directory as offering both medications for opioid use disorder and LGBTQ-specific treatment were confirmed as offering both services.
The availability of LGBTQ-specific services and medications for opioid use disorder varied by state
Among the 20 states with the highest rates of opioid-related overdose, less than 80% (n=43) of facilities in each of Missouri, New Mexico, Connecticut, and Illinois reported offering medications for opioid use disorder – which tended to be lower than other states. Over 30% (n=72) of facilitates in each of Michigan, New York, Massachusetts, and Missouri reported offering LGBTQ-specific services – which tended to be higher than most other states. Only New York, Massachusetts, and Missouri had more than 30% offering both medications for opioid use disorder and LGBTQ-specific services (n=58).
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that programs offering both opioid use disorder medications and tailored programming for the LGBTQ community are not widely available in many parts of the US. Although all the treatment facilities contacted by the authors had self-reported to SAMHSA that they offered both medications for opioid use disorder and LGBTQ-specific services, facility staff confirmed this was not the case for most treatment centers. The authors also found that the availability of these services varied regionally with states in the Northeastern US (New York and Massachusetts) having the highest availability of these services. Of note, however, over 30% of facilities contacted in Missouri also offered these services.
Taken together, these results may indicate that a noteworthy dearth of opioid use disorder services available to the LGBTQ community. This research builds upon previous work demonstrating discrepancies in theavailability of LGBTQ-specific treatment in the US. The fact that the availability of such services is so limited is concerning. LGBTQ-specific treatment programs are known to foster positive treatment outcomes for LGBTQ clients. The limited availability of such services represents a barrier to LGBTQ individuals from receiving effective care. That is, lower availability of LGBTQ-specific approaches in substance use disorder treatment settings may be a barrier to engaging with care. It is unclear exactly why such services are not widely available. One reason may be the absence of evidence-based protocols specifically for LGBTQ individuals with opioid use disorder. Future work is needed to understand what barriers facilities may encounter to implement inclusive care (e.g., operation costs, any contextual effects of low local LGBTQ population density, difficulty accessing evidence-based care designed for this group, etc.).
The current research cannot answer why discrepancies between listed and offered LGBTQ-specific services exist. It is possible that in some cases LGBTQ-specific programs may have been discontinued during the time between when representatives for the facilities reported their services to SAMHSA and when the facilities were contacted. This is somewhat supported in the article – the authors note that 4.3% of contacted facilities said that they had discontinued their LGBTQ-specific groups due to the COVID-19 pandemic. This does not account for the wide discrepancy between listed and offered services but does suggest that some treatment centers may have been forced to stop offering services due to extenuating circumstances. It is also possible that some of these facilities may have been attempting to market to a wider audience (i.e., the LGBTQ community). Regardless, the current study suggests that the way treatment facilities report what services they offer to SAMHSA would benefit from a closer look. A verification process, for example, may increase accuracy – which is important to understand treatment access facilitators and barriers for vulnerable groups like the LGBTQ community.
Unlike similar researchconducted previously, the current research did not examine availability of LGBTQ-specific opioid use disorder treatment across the entire US. Because the authors limited facilities to states with the top 20 highest opioid overdose rates, they may have missed valuable data from other states.
The study did not account for local LGBTQ-population density when assessing availability. That is, it seems possible that in some areas (particularly low population rural regions) the number of LGBTQ-identified people may be lower than states with more urban centers. As such, there likely would be less demand for specialized substance use disorder in such areas. It may have been more helpful for the authors to have employed some sort of weighting techniques to demonstrate availability of LGBTQ-specific services proportional to endemic LGBTQ populations.
BOTTOM LINE
This study found that there were discrepancies between the services listed on a national registry of substance use disorder treatment facilities and the available services at those facilities. Specifically, only ~24% of treatment facilities which reported to SAMHSA that they provided both medications for opioid use disorder and LGBTQ-specific reported that they had both types of these services when contacted directly. The authors also found that these discrepancies varied across states. Facilities in New York, Massachusetts, and Missouri had the highest congruence between listed and offered services. This study adds to the literature showing limited availability of opioid use disorder treatment specific to the needs of LGBTQ populations in the US. Expansion of such services are critical as they would be a vital tool in addressing LGBTQ opioid-related health disparities. It is critical for more research to be conducted demonstrating why medications for opioid use disorder and LGBT-specific services may not be more widely available.
For individuals and families seeking recovery: It may be challenging to find opioid use disorder treatment tailored to meet the needs of LGBTQ individuals. Importantly this study showed that even when treatment facilities list that they do offer such care – this may not be the case in practice. This suggests that those seeking recovery services for themselves or others need to be especially diligent in searching for services capable of meeting the unique needs of LGBTQ patients. For example, it may be more fruitful to research local providers to ensure they have experience working with the LGBT community and/or who have received special training in fields relevant for these populations (e.g., gender affirming care). Once potential programs or providers are identified, it could be beneficial to reach out to them directly to confirm they have the expertise needed to meet the needs of LGBTQ clients.
For treatment professionals and treatment systems: The present study suggests that LGBTQ individuals may encounter barriers to receiving effective opioid use disorder care. This is consistent with other similar work illustrating limited access to LGBTQ-specific substance use treatment in the US. It is critically important for providers to account for potential barriers members of the LGBTQ community face when accessing care (e.g., social stigma towards LGBTQ people). It would be useful for providers and their staff to assess their current care environment and determine how it may need to be modified to accommodate the needs of the LGBTQ community. This may include incorporating cultural humility practices into care.
For scientists: The field may benefit from research examining reasons why treatment facilities that offer medications for opioid use disorder do not also include LGBTQ-specific services. Determining what may be preventing these services from being implemented could help determine how to address barriers to LGBTQ-specific care implementation. For example, it is possible that implementing these programs may be too burdensome for smaller facilities with limited funding.
For policy makers: Policy makers may consider implementing programs to address the needs of patients in substance use treatment who are also members of the LGBTQ community. One solution could be to reduce barriers to substance use treatment (e.g., through Medicaid expansion). Furthermore, it may be valuable to offer incentives to treatment providers to pursue training in LGBTQ-specific care. For example, the American Medical Association provides continuing education in LGBTQ-relevant issues to medical care providers. Analogous programs for substance use treatment providers which offer course credits could lead to increased availability of LGBTQ-specific substance use treatment. Trainings like these could also reduce anti-LGBTQ bias within substance use treatment contexts.