Which medications increase the risk of overdose when added to buprenorphine and methadone?
Opioid medications like buprenorphine and methadone reduce illicit opioid use and overdose. Yet, because these medications tend to depress the central nervous system, combining them with certain other medications, especially those with similar depressant effects, may increase overdose. This study evaluated whether medications such as benzodiazepines increase risk for overdose when added to methadone and buprenorphine.
Opioids are central nervous system depressants that produce analgesic effects through reductions in neuronal firing in regions associated with the transmission of pain. At high doses, opioid use can cause suppression of neuronal activity necessary for basic functioning, such as breathing, and therefore increase risk of death.
Medications for opioid use disorder, such as methadone and buprenorphine, are first-line treatments for opioid use disorder and have been shown to reduce the risk of opioid overdose-related mortality. Medications for opioid use disorder like methadone and buprenorphine are known as opioid agonists, which bind to opioid receptor sites in the brain and block other opioids used while the medication is active. Opioid agonist medications are slower acting and less potent than opioids like heroin and are effective at reducing craving and withdrawal symptoms. Methadone is a full opioid agonist that is capable of binding to opioid receptor sites with greater affinity and is capable of triggering opioid overdose at higher doses. Buprenorphine is a partial opioid agonist and carries less overdose risk relative to methadone.
Patients being treated for opioid use disorder may be receiving treatment for co-occurring physical or psychiatric conditions that are common among people with substance use disorders, such as insomnia, depression or anxiety, chronic physical pain, or other substance use disorders. Some common medications for these co-occurring conditions include benzodiazepines, gabapentinoids, and Z-drugs (sleep medications like zolpidem better known by its brand name “Ambien”). These medications are also central nervous system depressants and have the effect of reducing activity in brain regions that maintain basic functioning. There is some evidence to suggest that the pharmacological effects of medications in these classes may interact with opioid agonists amplifying risk of overdose. This study evaluated the comparative safety of methadone and buprenorphine by examining additional risk for non-fatal overdose within the context of other medications commonly prescribed for people with opioid use disorder, including benzodiazepines, antipsychotics, anti- depressants, gabapentinoids, Z-drugs or opioids.
HOW WAS THIS STUDY CONDUCTED?
The study used a retrospective cohort study design with researchers extracting episodes of non-fatal overdose as identified by ICD-10 codes from longitudinal electronic health record data in a large database that accounts for almost 20% of the population of the United Kingdom. The study then examined differences in likelihood of non-fatal overdose use during periods of opioid agonist therapy alone compared to periods of opioid agonist therapy prescribed concurrently with other common medications (e.g., benzodiazepenes). Patients between the ages of 18 and 64 with 1 or more prescriptions of methadone or buprenorphine between 1998 and 2017 were included in the study cohort. Sample included 20,898 patients receiving opioid agonist medication.
The primary outcome of interest was episodes of non-fatal overdose as identified by ICD-10 codes that denoted mental and behavioral disorders due to psychoactive substances, accidental poisoning or self-harm, poisoning by drugs of undetermined intent, and poisoning by drugs including opioids.
The researchers were primarily interested in whether non-fatal overdoses were more likely during periods when patients were concurrently prescribed methadone or buprenorphine with any of the following: benzodiazepines (e.g., clonazepam known by the brand name Klonopin), antipsychotics (e.g., aripiprazole known by the brand name Abilify), anti-depressants (e.g., fluoxetine known by the brand name Prozac), gabapentinoids (e.g., gabapentin and pregabalin known by brand names Neurontin and Lyrica, respectively), Z-drugs (e.g., zolpidem known by the brand name Ambien), or opioids (e.g., oxycodone known for its extended release formulation branded as Oxycontin). For each patient, the researchers differentiated periods when an opioid agonist was used alone compared to when they were prescribed concurrently with one of the medications of interest. As a result, each patient contributed data for both periods, and the period in which they were only prescribed opioid agonist therapy served as the reference group for testing whether there was an additional risk of non-fatal overdose while prescribed another medication of interest concurrently. They also examined periods when patients were prescribed the medication but were not receiving opioid agonist therapy at the time.
The researchers carefully differentiated periods of active opioid agonist therapy only and concurrently prescribed with medications of interest. Periods of opioid agonist therapy were defined as the 14-day period after a prescription was issued, considering that in the United Kingdom an opioid agonist therapy is not allowed to exceed 14 days. Discontinuation periods were also identified, in which a prescription was not filled during an active opioid agonist therapy period, and active opioid agonist therapy periods resumed when a new prescription was issued. Three-fourths (72.5%) received a methadone prescription. If a patient switched medications, this began a new index episode of opioid agonist treatment where the study examined the presence or absence of other medications.
A similar approach was used to determine active period of use for the other prescribed medications of interest. The researchers defined treatment episodes of 7-day duration for benzodiazepines, Z-drugs or opioids and of 14-day duration for gabapentinoids, antipsychotics and antidepressants. Similar to opioid agonist therapy, continuous treatment was assumed following a new prescription within 7 to 14 days following the completion of the previous treatment episode. Note that the study design was not able to account statistically for whether participants took the medication as prescribed, only whether or not they filled a prescription.
The researchers adjusted their analyses statistically for gender, ethnicity, socioeconomic position, region of their general practitioner, heavy alcohol use based on presence in their medical record, history of overdose or self-harm, severe mental illness, prescriptions of benzodiazepines, gabapentinoids, antipsychotics or Z-drugs at baseline. The authors also include a time “period” variable (before or after 2010) to control for policy changes at those times. The researchers included these variables to increase their ability to determine any differences during periods of concurrent use of opioid agonist therapy and concurrent use of other prescriptions rather than to other factors.
WHAT DID THIS STUDY FIND?
Benzodiazepines, Antipsychotics, Gabapentinoids, and Z-Drugs Prescribed Concurrently with Opioid Agonists Associated with Increased Overdose Risk
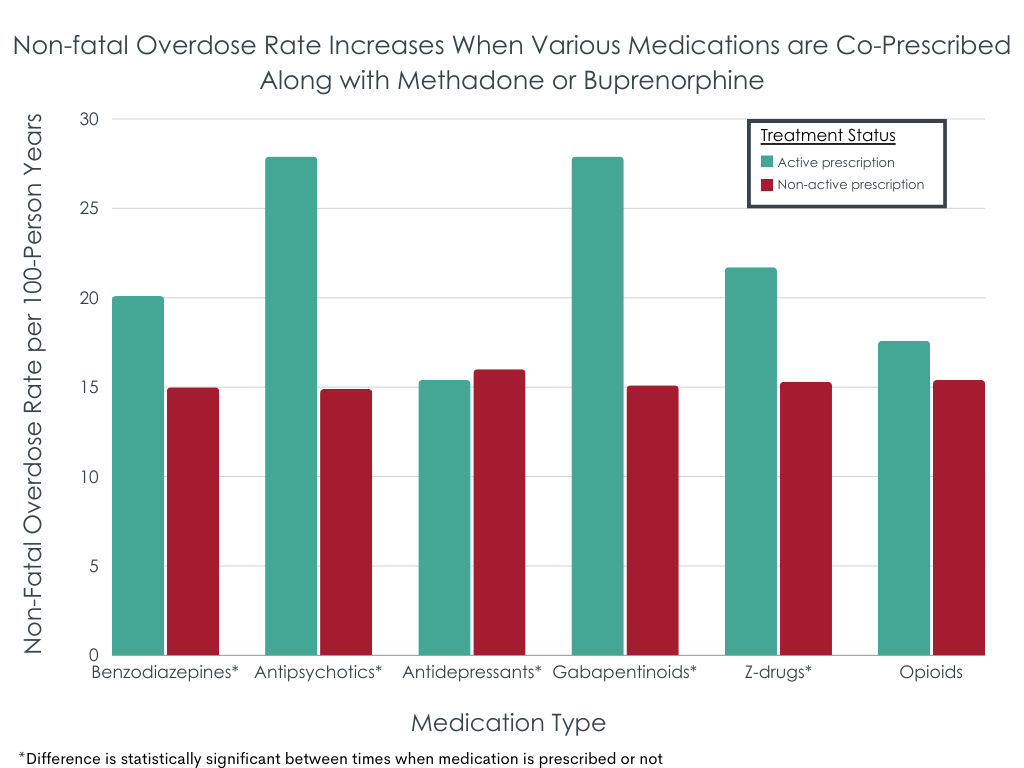
During the study period, there were 12,973 non-fatal overdose events (event rate = 15.47 per 100 person-years) resulting in hospital admission. Of these, 3,739 (29%) occurred during a period of prescription for at least one of the examined medications.
During periods of active opioid agonist prescription, non-fatal overdose event rates were significantly more likely during co-prescription of benzodiazepines (30% increase) antipsychotics (47% increase), gabapentinoids (49% increase), and Z-drugs (46% increase). The figure below illustrates overdose differences by the presence versus absence of each medication group. Co-prescription of antidepressants was associated with reduced non-fatal overdose risk. There was not a significant difference in non-fatal overdose risk when opioid agonists were co-prescribed with opioids.
Differences in Non-fatal Overdose When Prescribed Buprenorphine Compared to Methadone
A separate set of analyses examined whether, during times when patients were prescribed one of these common other medications, receiving or not receiving opioid agonist medication increase overdose risk. Somewhat unexpectedly, buprenorphine prescription tended to increase risk more than methadone. This was the case with benzodiazepines, antipsychotics, and gabapentinoids where buprenorphine prescription (compared to no prescription) was associated with a larger increase in risk for non-fatal overdose than methadone prescription or benzodiazepines and gabapentenoids. It is important to note that for both medications, times when receiving either buprenorphine or methadone increased risk for overdose compared to no medication, but buprenorphine increased it more.
As expected, however, methadone patients were more likely than buprenorphine patients to experience a non-fatal overdose event when co-prescribed Z-drugs and opioids. Of note, when opioids such as oxycodone were prescribed, having a buprenorphine prescription halved the overdose risk while having a methadone prescription increase risk by two-thirds.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study showed that among opioid use disorder patients receiving methadone or buprenorphine co-prescription with benzodiazepines, antipsychotics, gabapentinoids, or Z-drugs there was an association with increased risk of non-fatal overdose events. Alternatively, antidepressants were associated with reduced likelihood of non-fatal overdose risk events. These results are generally consistent with the literature on fatal overdose events during opioid agonist prescription, which suggest that co-prescription with benzodiazepines, Z-drugs or gabapentinoids represent an increased risk. The current study design does not capture adherence to the medication as prescribed, but rather measures non-fatal overdose events during periods of co-prescription. While it may be that these additional prescriptions are markers of greater periods of clinical acuity, during which overdose risk is likely to be greater, the risks for drowsiness, somnolence, and other indicators of slowed breathing suggest they are, in fact, potentiating agonist medications to increase overdose risk.
Also of note, co-prescription of anti-depressants was associated with lower overdose risk. It could be that antidepressants help improve quality of life and other aspects of recovery capital thereby reducing the likelihood of overdose – where antidepressants themselves may be indirectly accounting for the decreased risk through improvements in other areas of functioning. It might also be that antidepressants are a marker of health seeking overall (e.g., recovery support engagement, attention to diet and exercise, etc.), which improve well-being and reduce overdose risk. The reason that antipsychotics would not have this same association with healthier lifestyle behaviors is that some (but not all) do, in fact, potentiate the sedating effects of opioids to increase overdose risk, whereas antidepressants like fluoxetine (known by the brand name Prozac) and sertraline (known by the brand name Zoloft) are not known to potentiate the sedating effects of opioids.
It is important to note that risk of overdose events is significantly lower when prescribed methadone or buprenorphine relative to illicit use of other opioids, such as heroin or fentanyl, and that despite these risks, both medications represent major advances in the treatment of opioid use disorder.
That said, these results highlight the importance of considering other medications when making prescription decisions. Prescription Drug Monitoring Programs, which are large databases that monitor prescriptions, have the potential to help avoid these types of interactions. However, it is important to note that these programs may also sometimes impact willingness of prescribers to prescribe certain medications, such as opioids, to people with substance use disorders and co-occurring pain, which can prevent access to necessary care for some. Overall, greater attention to individual factors that differentially predict likelihood of overdose events may help tailor patient recommendations and treatment plans (i.e., precision medicine), including but not limited to decisions regarding other medications when patients are receiving agonist medications for opioid use disorder.
It is unclear why, in the current study, methadone generally increased risk to a lesser degree relative to buprenorphine when co-prescribed with certain medications. Methadone generally has a higher degree of overdose risk when taken alone due to its greater pharmacological strength as a full opioid agonist relative to buprenorphine which is a partial opioid agonist. The current study did not report on fatal overdose events, and it is possible that methadone in combination with other drugs may be associated with greater overall risk of overdose events, and more so fatal overdose events (due to its pharmacological profile), but reduced non-fatal overdose events. Further, given that buprenorphine was less commonly prescribed in this sample, there were in some cases limited numbers of total non-fatal overdose events during co-prescription of some of the medications of interest. As a result, there was more uncertainty about these findings (i.e., larger confidence intervals), and these analyses should be considered preliminary.
While the current study focused on co-prescription of medications, alcohol is also frequently used concurrently with other medications, in addition to opioid agonist therapy. Alcohol is another central nervous system depressant that can interact with these medications and may lead to increased likelihood of non-fatal overdose events. The analyses here controlled statistically for heavy alcohol use captured at baseline but did not measure alcohol use over time during these periods of opioid agonist treatment with and without co-prescription of other medications.
Fatal overdoses were not reported, and it is unclear whether these findings would be consistent when observing overall risk of both fatal and non-fatal overdose.
2. As mentioned above, the study design did not allow for consideration of whether patients took the medication as prescribed or not.
BOTTOM LINE
Among people prescribed buprenorphine or methadone, non-fatal overdose events are more likely when patients are also co-prescribed benzodiazepines, antipsychotics, gabapentinoids, and Z-drugs. Risk of overdose is significantly lower for those prescribed antidepressants, though this could be a marker of health seeking behaviors, generally, in the absence of opioid-potentiating risks like those present with some antipsychotic medications. Risk of non-fatal overdose may be greater when buprenorphine is co-prescribed with benzodiazepines, antipsychotics, or gabapentinoids, or when methadone is co-prescribed with Z-drugs or other opioids.
For individuals and families seeking recovery: If you or someone you know has been prescribed an opioid agonist, it may be important to review other prescribed medications to know whether there may be higher risk of an overdose event when these medications are used in combination amplifying sedative effects. Consider talking to your prescriber to determine all options that reduce risk while providing the greatest benefit. It is also important to take medications as prescribed in order to avoid adverse events.
For treatment professionals and treatment systems: Treatment for patients with opioid use disorder is likely to improve, and risk of overdose likely to reduce, if all treatment providers, including mental health clinicians or other non-prescribing providers, are aware of medications prescribed to their patients with opioid use disorder. Those prescribing opioid agonist therapy should be aware of the increased risk of non-fatal overdose when co-prescribed with the medications included in this study. Patient care may be improved if prescribers discuss risks of concurrent prescriptions at the initial prescribing session and at subsequent visits.
For scientists: More research is needed to understand pharmacological mechanisms that may increase overdose risk for each of these individual drug classes and to determine how to increase efficacy of opioid agonists while also reducing risk. There may also be individual differences among patients that differentially predict likelihood of overdose events. Knowledge of such factors may help tailor patient recommendations and treatment plans (i.e., precision medicine).
For policy makers: More funding would provide scientists the critical infrastructure to study how to reduce overdose events and to develop novel intervention approaches that are associated with decreased overall risk.
Opioids are central nervous system depressants that produce analgesic effects through reductions in neuronal firing in regions associated with the transmission of pain. At high doses, opioid use can cause suppression of neuronal activity necessary for basic functioning, such as breathing, and therefore increase risk of death.
Medications for opioid use disorder, such as methadone and buprenorphine, are first-line treatments for opioid use disorder and have been shown to reduce the risk of opioid overdose-related mortality. Medications for opioid use disorder like methadone and buprenorphine are known as opioid agonists, which bind to opioid receptor sites in the brain and block other opioids used while the medication is active. Opioid agonist medications are slower acting and less potent than opioids like heroin and are effective at reducing craving and withdrawal symptoms. Methadone is a full opioid agonist that is capable of binding to opioid receptor sites with greater affinity and is capable of triggering opioid overdose at higher doses. Buprenorphine is a partial opioid agonist and carries less overdose risk relative to methadone.
Patients being treated for opioid use disorder may be receiving treatment for co-occurring physical or psychiatric conditions that are common among people with substance use disorders, such as insomnia, depression or anxiety, chronic physical pain, or other substance use disorders. Some common medications for these co-occurring conditions include benzodiazepines, gabapentinoids, and Z-drugs (sleep medications like zolpidem better known by its brand name “Ambien”). These medications are also central nervous system depressants and have the effect of reducing activity in brain regions that maintain basic functioning. There is some evidence to suggest that the pharmacological effects of medications in these classes may interact with opioid agonists amplifying risk of overdose. This study evaluated the comparative safety of methadone and buprenorphine by examining additional risk for non-fatal overdose within the context of other medications commonly prescribed for people with opioid use disorder, including benzodiazepines, antipsychotics, anti- depressants, gabapentinoids, Z-drugs or opioids.
HOW WAS THIS STUDY CONDUCTED?
The study used a retrospective cohort study design with researchers extracting episodes of non-fatal overdose as identified by ICD-10 codes from longitudinal electronic health record data in a large database that accounts for almost 20% of the population of the United Kingdom. The study then examined differences in likelihood of non-fatal overdose use during periods of opioid agonist therapy alone compared to periods of opioid agonist therapy prescribed concurrently with other common medications (e.g., benzodiazepenes). Patients between the ages of 18 and 64 with 1 or more prescriptions of methadone or buprenorphine between 1998 and 2017 were included in the study cohort. Sample included 20,898 patients receiving opioid agonist medication.
The primary outcome of interest was episodes of non-fatal overdose as identified by ICD-10 codes that denoted mental and behavioral disorders due to psychoactive substances, accidental poisoning or self-harm, poisoning by drugs of undetermined intent, and poisoning by drugs including opioids.
The researchers were primarily interested in whether non-fatal overdoses were more likely during periods when patients were concurrently prescribed methadone or buprenorphine with any of the following: benzodiazepines (e.g., clonazepam known by the brand name Klonopin), antipsychotics (e.g., aripiprazole known by the brand name Abilify), anti-depressants (e.g., fluoxetine known by the brand name Prozac), gabapentinoids (e.g., gabapentin and pregabalin known by brand names Neurontin and Lyrica, respectively), Z-drugs (e.g., zolpidem known by the brand name Ambien), or opioids (e.g., oxycodone known for its extended release formulation branded as Oxycontin). For each patient, the researchers differentiated periods when an opioid agonist was used alone compared to when they were prescribed concurrently with one of the medications of interest. As a result, each patient contributed data for both periods, and the period in which they were only prescribed opioid agonist therapy served as the reference group for testing whether there was an additional risk of non-fatal overdose while prescribed another medication of interest concurrently. They also examined periods when patients were prescribed the medication but were not receiving opioid agonist therapy at the time.
The researchers carefully differentiated periods of active opioid agonist therapy only and concurrently prescribed with medications of interest. Periods of opioid agonist therapy were defined as the 14-day period after a prescription was issued, considering that in the United Kingdom an opioid agonist therapy is not allowed to exceed 14 days. Discontinuation periods were also identified, in which a prescription was not filled during an active opioid agonist therapy period, and active opioid agonist therapy periods resumed when a new prescription was issued. Three-fourths (72.5%) received a methadone prescription. If a patient switched medications, this began a new index episode of opioid agonist treatment where the study examined the presence or absence of other medications.
A similar approach was used to determine active period of use for the other prescribed medications of interest. The researchers defined treatment episodes of 7-day duration for benzodiazepines, Z-drugs or opioids and of 14-day duration for gabapentinoids, antipsychotics and antidepressants. Similar to opioid agonist therapy, continuous treatment was assumed following a new prescription within 7 to 14 days following the completion of the previous treatment episode. Note that the study design was not able to account statistically for whether participants took the medication as prescribed, only whether or not they filled a prescription.
The researchers adjusted their analyses statistically for gender, ethnicity, socioeconomic position, region of their general practitioner, heavy alcohol use based on presence in their medical record, history of overdose or self-harm, severe mental illness, prescriptions of benzodiazepines, gabapentinoids, antipsychotics or Z-drugs at baseline. The authors also include a time “period” variable (before or after 2010) to control for policy changes at those times. The researchers included these variables to increase their ability to determine any differences during periods of concurrent use of opioid agonist therapy and concurrent use of other prescriptions rather than to other factors.
WHAT DID THIS STUDY FIND?
Benzodiazepines, Antipsychotics, Gabapentinoids, and Z-Drugs Prescribed Concurrently with Opioid Agonists Associated with Increased Overdose Risk
During the study period, there were 12,973 non-fatal overdose events (event rate = 15.47 per 100 person-years) resulting in hospital admission. Of these, 3,739 (29%) occurred during a period of prescription for at least one of the examined medications.
During periods of active opioid agonist prescription, non-fatal overdose event rates were significantly more likely during co-prescription of benzodiazepines (30% increase) antipsychotics (47% increase), gabapentinoids (49% increase), and Z-drugs (46% increase). The figure below illustrates overdose differences by the presence versus absence of each medication group. Co-prescription of antidepressants was associated with reduced non-fatal overdose risk. There was not a significant difference in non-fatal overdose risk when opioid agonists were co-prescribed with opioids.
Differences in Non-fatal Overdose When Prescribed Buprenorphine Compared to Methadone
A separate set of analyses examined whether, during times when patients were prescribed one of these common other medications, receiving or not receiving opioid agonist medication increase overdose risk. Somewhat unexpectedly, buprenorphine prescription tended to increase risk more than methadone. This was the case with benzodiazepines, antipsychotics, and gabapentinoids where buprenorphine prescription (compared to no prescription) was associated with a larger increase in risk for non-fatal overdose than methadone prescription or benzodiazepines and gabapentenoids. It is important to note that for both medications, times when receiving either buprenorphine or methadone increased risk for overdose compared to no medication, but buprenorphine increased it more.
As expected, however, methadone patients were more likely than buprenorphine patients to experience a non-fatal overdose event when co-prescribed Z-drugs and opioids. Of note, when opioids such as oxycodone were prescribed, having a buprenorphine prescription halved the overdose risk while having a methadone prescription increase risk by two-thirds.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study showed that among opioid use disorder patients receiving methadone or buprenorphine co-prescription with benzodiazepines, antipsychotics, gabapentinoids, or Z-drugs there was an association with increased risk of non-fatal overdose events. Alternatively, antidepressants were associated with reduced likelihood of non-fatal overdose risk events. These results are generally consistent with the literature on fatal overdose events during opioid agonist prescription, which suggest that co-prescription with benzodiazepines, Z-drugs or gabapentinoids represent an increased risk. The current study design does not capture adherence to the medication as prescribed, but rather measures non-fatal overdose events during periods of co-prescription. While it may be that these additional prescriptions are markers of greater periods of clinical acuity, during which overdose risk is likely to be greater, the risks for drowsiness, somnolence, and other indicators of slowed breathing suggest they are, in fact, potentiating agonist medications to increase overdose risk.
Also of note, co-prescription of anti-depressants was associated with lower overdose risk. It could be that antidepressants help improve quality of life and other aspects of recovery capital thereby reducing the likelihood of overdose – where antidepressants themselves may be indirectly accounting for the decreased risk through improvements in other areas of functioning. It might also be that antidepressants are a marker of health seeking overall (e.g., recovery support engagement, attention to diet and exercise, etc.), which improve well-being and reduce overdose risk. The reason that antipsychotics would not have this same association with healthier lifestyle behaviors is that some (but not all) do, in fact, potentiate the sedating effects of opioids to increase overdose risk, whereas antidepressants like fluoxetine (known by the brand name Prozac) and sertraline (known by the brand name Zoloft) are not known to potentiate the sedating effects of opioids.
It is important to note that risk of overdose events is significantly lower when prescribed methadone or buprenorphine relative to illicit use of other opioids, such as heroin or fentanyl, and that despite these risks, both medications represent major advances in the treatment of opioid use disorder.
That said, these results highlight the importance of considering other medications when making prescription decisions. Prescription Drug Monitoring Programs, which are large databases that monitor prescriptions, have the potential to help avoid these types of interactions. However, it is important to note that these programs may also sometimes impact willingness of prescribers to prescribe certain medications, such as opioids, to people with substance use disorders and co-occurring pain, which can prevent access to necessary care for some. Overall, greater attention to individual factors that differentially predict likelihood of overdose events may help tailor patient recommendations and treatment plans (i.e., precision medicine), including but not limited to decisions regarding other medications when patients are receiving agonist medications for opioid use disorder.
It is unclear why, in the current study, methadone generally increased risk to a lesser degree relative to buprenorphine when co-prescribed with certain medications. Methadone generally has a higher degree of overdose risk when taken alone due to its greater pharmacological strength as a full opioid agonist relative to buprenorphine which is a partial opioid agonist. The current study did not report on fatal overdose events, and it is possible that methadone in combination with other drugs may be associated with greater overall risk of overdose events, and more so fatal overdose events (due to its pharmacological profile), but reduced non-fatal overdose events. Further, given that buprenorphine was less commonly prescribed in this sample, there were in some cases limited numbers of total non-fatal overdose events during co-prescription of some of the medications of interest. As a result, there was more uncertainty about these findings (i.e., larger confidence intervals), and these analyses should be considered preliminary.
While the current study focused on co-prescription of medications, alcohol is also frequently used concurrently with other medications, in addition to opioid agonist therapy. Alcohol is another central nervous system depressant that can interact with these medications and may lead to increased likelihood of non-fatal overdose events. The analyses here controlled statistically for heavy alcohol use captured at baseline but did not measure alcohol use over time during these periods of opioid agonist treatment with and without co-prescription of other medications.
Fatal overdoses were not reported, and it is unclear whether these findings would be consistent when observing overall risk of both fatal and non-fatal overdose.
2. As mentioned above, the study design did not allow for consideration of whether patients took the medication as prescribed or not.
BOTTOM LINE
Among people prescribed buprenorphine or methadone, non-fatal overdose events are more likely when patients are also co-prescribed benzodiazepines, antipsychotics, gabapentinoids, and Z-drugs. Risk of overdose is significantly lower for those prescribed antidepressants, though this could be a marker of health seeking behaviors, generally, in the absence of opioid-potentiating risks like those present with some antipsychotic medications. Risk of non-fatal overdose may be greater when buprenorphine is co-prescribed with benzodiazepines, antipsychotics, or gabapentinoids, or when methadone is co-prescribed with Z-drugs or other opioids.
For individuals and families seeking recovery: If you or someone you know has been prescribed an opioid agonist, it may be important to review other prescribed medications to know whether there may be higher risk of an overdose event when these medications are used in combination amplifying sedative effects. Consider talking to your prescriber to determine all options that reduce risk while providing the greatest benefit. It is also important to take medications as prescribed in order to avoid adverse events.
For treatment professionals and treatment systems: Treatment for patients with opioid use disorder is likely to improve, and risk of overdose likely to reduce, if all treatment providers, including mental health clinicians or other non-prescribing providers, are aware of medications prescribed to their patients with opioid use disorder. Those prescribing opioid agonist therapy should be aware of the increased risk of non-fatal overdose when co-prescribed with the medications included in this study. Patient care may be improved if prescribers discuss risks of concurrent prescriptions at the initial prescribing session and at subsequent visits.
For scientists: More research is needed to understand pharmacological mechanisms that may increase overdose risk for each of these individual drug classes and to determine how to increase efficacy of opioid agonists while also reducing risk. There may also be individual differences among patients that differentially predict likelihood of overdose events. Knowledge of such factors may help tailor patient recommendations and treatment plans (i.e., precision medicine).
For policy makers: More funding would provide scientists the critical infrastructure to study how to reduce overdose events and to develop novel intervention approaches that are associated with decreased overall risk.
Opioids are central nervous system depressants that produce analgesic effects through reductions in neuronal firing in regions associated with the transmission of pain. At high doses, opioid use can cause suppression of neuronal activity necessary for basic functioning, such as breathing, and therefore increase risk of death.
Medications for opioid use disorder, such as methadone and buprenorphine, are first-line treatments for opioid use disorder and have been shown to reduce the risk of opioid overdose-related mortality. Medications for opioid use disorder like methadone and buprenorphine are known as opioid agonists, which bind to opioid receptor sites in the brain and block other opioids used while the medication is active. Opioid agonist medications are slower acting and less potent than opioids like heroin and are effective at reducing craving and withdrawal symptoms. Methadone is a full opioid agonist that is capable of binding to opioid receptor sites with greater affinity and is capable of triggering opioid overdose at higher doses. Buprenorphine is a partial opioid agonist and carries less overdose risk relative to methadone.
Patients being treated for opioid use disorder may be receiving treatment for co-occurring physical or psychiatric conditions that are common among people with substance use disorders, such as insomnia, depression or anxiety, chronic physical pain, or other substance use disorders. Some common medications for these co-occurring conditions include benzodiazepines, gabapentinoids, and Z-drugs (sleep medications like zolpidem better known by its brand name “Ambien”). These medications are also central nervous system depressants and have the effect of reducing activity in brain regions that maintain basic functioning. There is some evidence to suggest that the pharmacological effects of medications in these classes may interact with opioid agonists amplifying risk of overdose. This study evaluated the comparative safety of methadone and buprenorphine by examining additional risk for non-fatal overdose within the context of other medications commonly prescribed for people with opioid use disorder, including benzodiazepines, antipsychotics, anti- depressants, gabapentinoids, Z-drugs or opioids.
HOW WAS THIS STUDY CONDUCTED?
The study used a retrospective cohort study design with researchers extracting episodes of non-fatal overdose as identified by ICD-10 codes from longitudinal electronic health record data in a large database that accounts for almost 20% of the population of the United Kingdom. The study then examined differences in likelihood of non-fatal overdose use during periods of opioid agonist therapy alone compared to periods of opioid agonist therapy prescribed concurrently with other common medications (e.g., benzodiazepenes). Patients between the ages of 18 and 64 with 1 or more prescriptions of methadone or buprenorphine between 1998 and 2017 were included in the study cohort. Sample included 20,898 patients receiving opioid agonist medication.
The primary outcome of interest was episodes of non-fatal overdose as identified by ICD-10 codes that denoted mental and behavioral disorders due to psychoactive substances, accidental poisoning or self-harm, poisoning by drugs of undetermined intent, and poisoning by drugs including opioids.
The researchers were primarily interested in whether non-fatal overdoses were more likely during periods when patients were concurrently prescribed methadone or buprenorphine with any of the following: benzodiazepines (e.g., clonazepam known by the brand name Klonopin), antipsychotics (e.g., aripiprazole known by the brand name Abilify), anti-depressants (e.g., fluoxetine known by the brand name Prozac), gabapentinoids (e.g., gabapentin and pregabalin known by brand names Neurontin and Lyrica, respectively), Z-drugs (e.g., zolpidem known by the brand name Ambien), or opioids (e.g., oxycodone known for its extended release formulation branded as Oxycontin). For each patient, the researchers differentiated periods when an opioid agonist was used alone compared to when they were prescribed concurrently with one of the medications of interest. As a result, each patient contributed data for both periods, and the period in which they were only prescribed opioid agonist therapy served as the reference group for testing whether there was an additional risk of non-fatal overdose while prescribed another medication of interest concurrently. They also examined periods when patients were prescribed the medication but were not receiving opioid agonist therapy at the time.
The researchers carefully differentiated periods of active opioid agonist therapy only and concurrently prescribed with medications of interest. Periods of opioid agonist therapy were defined as the 14-day period after a prescription was issued, considering that in the United Kingdom an opioid agonist therapy is not allowed to exceed 14 days. Discontinuation periods were also identified, in which a prescription was not filled during an active opioid agonist therapy period, and active opioid agonist therapy periods resumed when a new prescription was issued. Three-fourths (72.5%) received a methadone prescription. If a patient switched medications, this began a new index episode of opioid agonist treatment where the study examined the presence or absence of other medications.
A similar approach was used to determine active period of use for the other prescribed medications of interest. The researchers defined treatment episodes of 7-day duration for benzodiazepines, Z-drugs or opioids and of 14-day duration for gabapentinoids, antipsychotics and antidepressants. Similar to opioid agonist therapy, continuous treatment was assumed following a new prescription within 7 to 14 days following the completion of the previous treatment episode. Note that the study design was not able to account statistically for whether participants took the medication as prescribed, only whether or not they filled a prescription.
The researchers adjusted their analyses statistically for gender, ethnicity, socioeconomic position, region of their general practitioner, heavy alcohol use based on presence in their medical record, history of overdose or self-harm, severe mental illness, prescriptions of benzodiazepines, gabapentinoids, antipsychotics or Z-drugs at baseline. The authors also include a time “period” variable (before or after 2010) to control for policy changes at those times. The researchers included these variables to increase their ability to determine any differences during periods of concurrent use of opioid agonist therapy and concurrent use of other prescriptions rather than to other factors.
WHAT DID THIS STUDY FIND?
Benzodiazepines, Antipsychotics, Gabapentinoids, and Z-Drugs Prescribed Concurrently with Opioid Agonists Associated with Increased Overdose Risk
During the study period, there were 12,973 non-fatal overdose events (event rate = 15.47 per 100 person-years) resulting in hospital admission. Of these, 3,739 (29%) occurred during a period of prescription for at least one of the examined medications.
During periods of active opioid agonist prescription, non-fatal overdose event rates were significantly more likely during co-prescription of benzodiazepines (30% increase) antipsychotics (47% increase), gabapentinoids (49% increase), and Z-drugs (46% increase). The figure below illustrates overdose differences by the presence versus absence of each medication group. Co-prescription of antidepressants was associated with reduced non-fatal overdose risk. There was not a significant difference in non-fatal overdose risk when opioid agonists were co-prescribed with opioids.
Differences in Non-fatal Overdose When Prescribed Buprenorphine Compared to Methadone
A separate set of analyses examined whether, during times when patients were prescribed one of these common other medications, receiving or not receiving opioid agonist medication increase overdose risk. Somewhat unexpectedly, buprenorphine prescription tended to increase risk more than methadone. This was the case with benzodiazepines, antipsychotics, and gabapentinoids where buprenorphine prescription (compared to no prescription) was associated with a larger increase in risk for non-fatal overdose than methadone prescription or benzodiazepines and gabapentenoids. It is important to note that for both medications, times when receiving either buprenorphine or methadone increased risk for overdose compared to no medication, but buprenorphine increased it more.
As expected, however, methadone patients were more likely than buprenorphine patients to experience a non-fatal overdose event when co-prescribed Z-drugs and opioids. Of note, when opioids such as oxycodone were prescribed, having a buprenorphine prescription halved the overdose risk while having a methadone prescription increase risk by two-thirds.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
This study showed that among opioid use disorder patients receiving methadone or buprenorphine co-prescription with benzodiazepines, antipsychotics, gabapentinoids, or Z-drugs there was an association with increased risk of non-fatal overdose events. Alternatively, antidepressants were associated with reduced likelihood of non-fatal overdose risk events. These results are generally consistent with the literature on fatal overdose events during opioid agonist prescription, which suggest that co-prescription with benzodiazepines, Z-drugs or gabapentinoids represent an increased risk. The current study design does not capture adherence to the medication as prescribed, but rather measures non-fatal overdose events during periods of co-prescription. While it may be that these additional prescriptions are markers of greater periods of clinical acuity, during which overdose risk is likely to be greater, the risks for drowsiness, somnolence, and other indicators of slowed breathing suggest they are, in fact, potentiating agonist medications to increase overdose risk.
Also of note, co-prescription of anti-depressants was associated with lower overdose risk. It could be that antidepressants help improve quality of life and other aspects of recovery capital thereby reducing the likelihood of overdose – where antidepressants themselves may be indirectly accounting for the decreased risk through improvements in other areas of functioning. It might also be that antidepressants are a marker of health seeking overall (e.g., recovery support engagement, attention to diet and exercise, etc.), which improve well-being and reduce overdose risk. The reason that antipsychotics would not have this same association with healthier lifestyle behaviors is that some (but not all) do, in fact, potentiate the sedating effects of opioids to increase overdose risk, whereas antidepressants like fluoxetine (known by the brand name Prozac) and sertraline (known by the brand name Zoloft) are not known to potentiate the sedating effects of opioids.
It is important to note that risk of overdose events is significantly lower when prescribed methadone or buprenorphine relative to illicit use of other opioids, such as heroin or fentanyl, and that despite these risks, both medications represent major advances in the treatment of opioid use disorder.
That said, these results highlight the importance of considering other medications when making prescription decisions. Prescription Drug Monitoring Programs, which are large databases that monitor prescriptions, have the potential to help avoid these types of interactions. However, it is important to note that these programs may also sometimes impact willingness of prescribers to prescribe certain medications, such as opioids, to people with substance use disorders and co-occurring pain, which can prevent access to necessary care for some. Overall, greater attention to individual factors that differentially predict likelihood of overdose events may help tailor patient recommendations and treatment plans (i.e., precision medicine), including but not limited to decisions regarding other medications when patients are receiving agonist medications for opioid use disorder.
It is unclear why, in the current study, methadone generally increased risk to a lesser degree relative to buprenorphine when co-prescribed with certain medications. Methadone generally has a higher degree of overdose risk when taken alone due to its greater pharmacological strength as a full opioid agonist relative to buprenorphine which is a partial opioid agonist. The current study did not report on fatal overdose events, and it is possible that methadone in combination with other drugs may be associated with greater overall risk of overdose events, and more so fatal overdose events (due to its pharmacological profile), but reduced non-fatal overdose events. Further, given that buprenorphine was less commonly prescribed in this sample, there were in some cases limited numbers of total non-fatal overdose events during co-prescription of some of the medications of interest. As a result, there was more uncertainty about these findings (i.e., larger confidence intervals), and these analyses should be considered preliminary.
While the current study focused on co-prescription of medications, alcohol is also frequently used concurrently with other medications, in addition to opioid agonist therapy. Alcohol is another central nervous system depressant that can interact with these medications and may lead to increased likelihood of non-fatal overdose events. The analyses here controlled statistically for heavy alcohol use captured at baseline but did not measure alcohol use over time during these periods of opioid agonist treatment with and without co-prescription of other medications.
Fatal overdoses were not reported, and it is unclear whether these findings would be consistent when observing overall risk of both fatal and non-fatal overdose.
2. As mentioned above, the study design did not allow for consideration of whether patients took the medication as prescribed or not.
BOTTOM LINE
Among people prescribed buprenorphine or methadone, non-fatal overdose events are more likely when patients are also co-prescribed benzodiazepines, antipsychotics, gabapentinoids, and Z-drugs. Risk of overdose is significantly lower for those prescribed antidepressants, though this could be a marker of health seeking behaviors, generally, in the absence of opioid-potentiating risks like those present with some antipsychotic medications. Risk of non-fatal overdose may be greater when buprenorphine is co-prescribed with benzodiazepines, antipsychotics, or gabapentinoids, or when methadone is co-prescribed with Z-drugs or other opioids.
For individuals and families seeking recovery: If you or someone you know has been prescribed an opioid agonist, it may be important to review other prescribed medications to know whether there may be higher risk of an overdose event when these medications are used in combination amplifying sedative effects. Consider talking to your prescriber to determine all options that reduce risk while providing the greatest benefit. It is also important to take medications as prescribed in order to avoid adverse events.
For treatment professionals and treatment systems: Treatment for patients with opioid use disorder is likely to improve, and risk of overdose likely to reduce, if all treatment providers, including mental health clinicians or other non-prescribing providers, are aware of medications prescribed to their patients with opioid use disorder. Those prescribing opioid agonist therapy should be aware of the increased risk of non-fatal overdose when co-prescribed with the medications included in this study. Patient care may be improved if prescribers discuss risks of concurrent prescriptions at the initial prescribing session and at subsequent visits.
For scientists: More research is needed to understand pharmacological mechanisms that may increase overdose risk for each of these individual drug classes and to determine how to increase efficacy of opioid agonists while also reducing risk. There may also be individual differences among patients that differentially predict likelihood of overdose events. Knowledge of such factors may help tailor patient recommendations and treatment plans (i.e., precision medicine).
For policy makers: More funding would provide scientists the critical infrastructure to study how to reduce overdose events and to develop novel intervention approaches that are associated with decreased overall risk.