
Who Is Most Likely to Benefit from Moderation-focused Alcohol Treatment?
While the burden to deliver effective treatments falls on health care providers, individual factors can impact how well someone responds to these treatments. Among the most widely studied are how motivated and confident someone is in being able to reduce or quit drinking. Given the field’s historical emphasis on abstinence-based approaches, key individual factors to treatment outcome remain more of a mystery when it comes to moderation-focused treatment, sometimes called “harm reduction”.
Can we tell who is more likely to respond positively to moderation-focused treatment for alcohol use disorder?
WHAT PROBLEM DOES THIS STUDY ADDRESS?
There is a general consensus stemming from both clinical wisdom and scientific investigation that how motivated someone is to abstain from alcohol and other drugs, and how confident someone is in being able to abstain (i.e., self-efficacy), relates to better response to treatment, and often to longer-term outcomes as well.
Many individuals with an alcohol use disorder that wish to change their drinking, however, have a goal of moderation – sometimes referred to as “harm reduction” – rather than complete abstinence. Indeed, moderation appears to be a viable pathway to alcohol use disorder remission for some. Identifying who will be most likely to respond to these moderation-focused alcohol treatments will be key to clinical recommendations and policies related to moderation versus abstinence.
This study by Kuerbis and colleagues investigated how individuals with different clinical profiles will respond to moderation-focused alcohol interventions.
HOW WAS THIS STUDY CONDUCTED?
Study authors used data from their prior randomized trial that tested two motivational interventions and one comparison condition where individuals were simply encouraged to reduce their drinking taking place over 7 weeks. In order to be included in that original study, an individual had to be diagnosed with an alcohol use disorder, report a minimum average weekly drinking of 16+ drinks for women and 25+ for men, and express interest in a moderation approach to changing their drinking.
From this trial, 84 individuals were categorized using a sophisticated analytic approach into one of 3 groups based on daily assessments of their motivation & confidence related to drinking change during the week before beginning treatment:
* Heavy drinking was defined as 5 or more drinks in 1 day for women & 6 or more for men.
- High confidence to resist heavy drinking*, high commitment to reduce heavy drinking, and high commitment to abstain from alcohol (“High” group; n = 12)
- Moderate confidence to resist heavy drinking, high commitment to reduce heavy drinking, lower commitment to abstain from alcohol (“Moderate” group; n = 38)
- Low confidence to resist heavy drinking, low commitment to reduce heavy drinking, low commitment to abstain alcohol (“Low” group; n = 33)
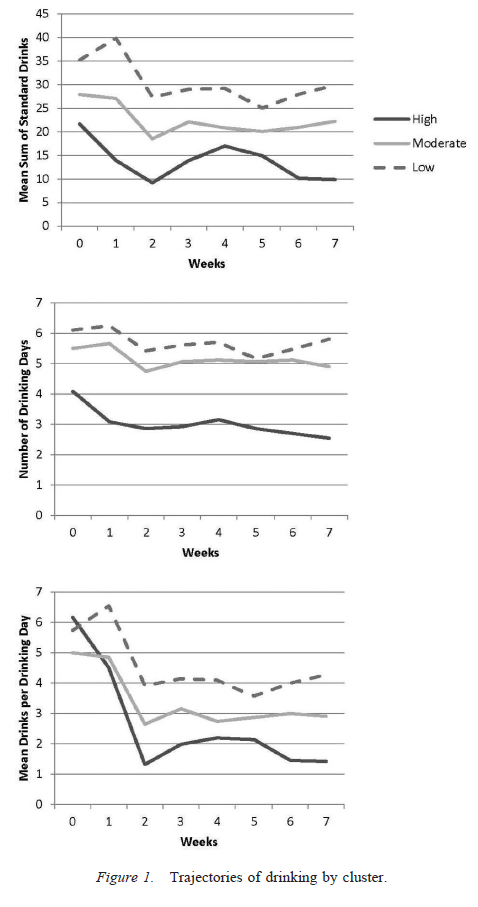
These three groups were compared on the following three outcomes each week over the course of the 7-week treatment period:
- total number of drinks per week
- number of drinking days per week
- number of drinks per drinking day each week
Important characteristics of the sample were that, before treatment, they had an average of four alcohol dependence criteria (based the fourth edition of the diagnostic and statistical manual of mental disorders, or DSM-IV), 5.5 drinking days per week (standard deviation = 1.7), 30 total drinks per week (standard deviation = 19.2) and a score of 6 on the genetic risk indicator where individuals received 2 for a parent or sibling with an alcohol or other drug problem and 1 for another type of relative. They were 40 years old, on average, and approximately half were female.
WHAT DID THIS STUDY FIND?
NOTABLY FROM THE STUDY:
- For total number of drinks per week, the High group had significantly greater reductions over the 7-week treatment period than both the Moderate (20% greater) and Low groups (28% greater), while the Moderate group also had greater reduction than the Low group.
- For total drinking days per week, the High group had significantly greater reduction than the Moderate group (19% greater) and the Low group (20%) while the Moderate and Low groups had similar reductions.
- For drinks per drinking day, the High group had significantly greater reduction than the Moderate (19%) and Low group (20%), while the Moderate group also had significantly greater reduction than the Low group.
When considered as an entire sample of 84 individuals, participants evidenced significant reductions in all three outcomes over the 7 week intervention period (total drinks, drinking days, and drinks per drinking day). Interestingly, analyses conducted after the main analyses to explore and learn more about the findings (i.e., “post-hoc” analyses) categorized individuals just according to their motivation to reduce heavy drinking and to abstain from alcohol; here the groups were not different in terms of their treatment response.
This indicates that participants’ confidence to reduce heavy drinking was particularly important to being able to predict how they responded to treatment.
It is also worth mentioning some baseline (i.e., pre-treatment) differences between the three groups to get a sense of the types of individuals in each group. The Low group had a greater percentage of individuals with the maximum possible score on an alcohol problem screening tool compared to Medium and High groups (79% vs. 37% vs. 46%) as well as greater percentage who had received alcohol use disorder treatment in the past (33% vs. 8% vs. 15%).
Although not quite reaching statistical significance (i.e., less reliable results due to the study’s smaller sample), the High group had a greater reported family history of drinking and other drug problems (5 vs. 5 for Low and Moderate vs. 8 for High).
WHY IS THIS STUDY IMPORTANT
Motivation & confidence are important psychological variables in treatment for alcohol use disorder, with confidence appearing to be especially key.
Individuals confident in their ability to reduce heavy drinking are most likely to respond well to a moderation-focused treatment and, as authors point out, they may be more willing to try abstaining on certain days to reach their overall moderation goal.
They not only had a greater reduction in drinking days per week (about 3 days per week by the end of the treatment period). Also interesting that, as the study authors point out, all groups improved to varying degrees particularly in terms of fewer drinks per drinking day.
These individuals notably made up just 14% of the sample, the smallest group of the three. At least based on these data, they are likely to make up a minor sub-set of individuals who seek moderation-focused treatment.
As authors point out, all groups improved to varying degrees particularly in terms of fewer drinks per drinking day, despite the fact that new skills to reduce or abstain were not an explicit part of any of the three treatments in the initial randomized trial. These individuals may be naturally finding ways in their environment to help them reduce or abstain (e.g., seeking social support), for example, or automatically using cognitive strategies to help them stick to limits on days they drink.
- LIMITATIONS
-
- The study was based on a small sample of just 84 individuals interested in moderating but not abstaining from alcohol use. They were drinking relatively small amounts, on average, compared to other study clinical treatment samples for alcohol use disorder (e.g., Project MATCH outpatients – those recruited directly from the community — were drinking about 65 drinks per week, on average, at the time of entering the study). That specific focus of the study is important to keep in mind.
- Also, the study should be replicated in a different setting with a larger sample before we can have confidence these findings can be applied to individuals with alcohol use disorder seeking moderation-focused treatment more generally.
- NEXT STEPS
-
- More work is needed on what psychological and social processes explain benefit from moderation-focused treatment as was done in the initial randomized trial. In other words, we need to answer these questions: “How is this treatment helpful? What explains whether someone benefits or not?”.
- Also, given research showing moderation is certainly a viable, but less stable (i.e., more risky) form of alcohol use disorder remission, it is important to see whether these individuals continue to use at less-harmful levels over the long-term without increasing drinking and related risks – and what characteristics help predict this longer-term positive response to moderation-focused treatment.
- In addition, it may be interesting to use a sequential research design that investigates if poor responders to moderation-focused treatment do better in an abstinence-focused approach.
- Lastly, the Low group is an especially interesting group. They came into the study with low motivation and confidence, and greater proportions were heavy drinkers and had been to alcohol use disorder treatment before. They could have been less hopeful that their drinking would improve – in other words, more pessimistic about their chances to make a meaningful change in their drinking. While the reasons for this pessimism are not entirely clear, more research needs to be done on this group, including why they are seeking moderation-focused treatment, and whether an abstinence-based approach might be more appropriate for these heavier drinkers.
BOTTOM LINE
- For individuals & families seeking recovery: You or your loved one’s short-term positive response to treatment for alcohol use disorder that helps individuals moderate their drinking, rather than abstain, may depend, in part, on having a less severe drinking problem initially and high confidence to be able to reduce the times where you drink heavily (5 or more drinks for a man and 4 or more for a woman).
- For Scientists: This small study provided interesting data on who will respond best to treatment aiming to help individuals moderate their drinking. Confidence to reduce heavy drinking pre-treatment appears to be especially important to treatment response. Given the small sample size, however, it is recommended that the results are considered in the spirit of hypothesis generation rather than hypothesis testing.
- For Policy makers: This study provides preliminary information showing confidence to reduce heavy drinking may be an important factor in response to moderation-focused treatment. However the results need to be replicated in different settings and with a larger sample. Research that can determine which individuals are most likely to benefit from moderation-focused approaches to alcohol use disorder treatment would be help address societal costs associated with harmful drinking, including health care, criminal justice, and lost work productivity costs.
- For Treatment professionals and treatment systems: This study provides preliminary information showing confidence to reduce heavy drinking may be an important factor in response to moderation-focused treatment. A thorough assessment of your patients’ confidence and motivation to reduce their heavy drinking could help determine which individuals would be more likely to respond positively in the short-term to moderation-focused treatment. In addition, it is important to keep in mind that the patients examined here had relatively mild to moderate drinking histories, on average, compared to individuals that typically participate in clinical research trials for alcohol use disorder psychosocial interventions. As such, alcohol use disorder severity (e.g., drinks per week, dependence symptoms, prior treatment) is important to consider as well when thinking about potential positive response to moderation-focused treatment. Overall, this research is still in early stages and more studies are needed to build on these initial findings.
CITATIONS
Kuerbis, A., Armeli, S., Muench, F., & Morgenstern, J. (2014). Profiles of confidence and commitment to change as predictors of moderated drinking: A person-centered approach. Psychology of Addictive Behaviors, 28(4), 1065.
