Women living with HIV use drugs less often than HIV negative women but seek drug use treatment just as much
Drug use disorder treatment is critical for improving health among people living with HIV. Rates of treatment utilization and corresponding health outcomes among women living with HIV is not as well understood as those of men. To help inform the unique needs of women with HIV, this study examined patterns of drug use and treatment among a sample of women with HIV.
To date the scope of drug use and treatment utilization among women with HIV is not well understood, which is particularly problematic given their unique health needs. It is plausible that rates of substance use disorder treatment among women with HIV are lower than the general population of people living with HIV since they experience additional barriers to substance use disorder treatment access. For instance, women with HIV face increased social stigmatization when seeking out treatment compared to people without HIV and face potential loss of parental custody. These barriers underscore the necessity of specific interventions designed to facilitate treatment among women with HIV who use drugs. To inform such interventions, the current study examined patterns of drug use and treatment utilization among a sample of women.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the Women’s Interagency HIV Study (WIHS). This prospective cohort study began in 1993 to monitor the health of women with HIV and women at risk of contracting HIV. Participants were recruited from 10 sites across the US (Bronx, NY, Brooklyn, NY, Chicago, IL, Los Angeles, CA, Miami, FL, Atlanta, GA, Chapel Hill, NC, Birmingham, AL, Jackson, MS, and the District of Columbia). The WIHS has since merged with the Multicenter AIDS Cohort Study (MACS) and is now known as the MACS-WIHS Combined Cohort Study (MACS-WIHS CCS). Data for the current analysis came from participants who completed a baseline visit and at least one follow-up visit from October 2013 – March 2020.
Participants in the current analysis (1802 women with HIV and 757 HIV negative women) came from multiple cohorts recruited throughout the WIHS project’s lifespan. Initial inclusion criteria were: (1) 18+ years old; (2) female; (3) able to complete an interview in English or Spanish; (4) able to travel to research site every 6 months for an interview/examination/blood draw. These criteria were later expanded in 2001 to recruit more HIV positive women and women at risk of contracting HIV. These additional criteria included: (i) proof of HIV serostatus (e.g., documented results from an HIV enzyme-linked immunosorbent assay) obtained within 30 days prior to enrollment and a confirmatory HIV test; (ii) no history of clinical AIDS-related conditions (confirmed via medical records); (iii) documentation of laboratory reports of HIV RNA levels and CD4 counts surrounding the period of HIV medication initiation for those on HIV medications; and (iv) consent to have specimens stored in the WIHS national repository. In addition, to ensure recruited HIV negative women were at risk of contracting HIV, the researchers included HIV negative women who reported one or more of the following: (a) injection drug use; (b) having a sexually transmitted disease (sans HIV); (c) having unprotected sex with three or more men or protected sex with more than five men; or (d) having exchanged sex for drugs, money, or shelter.
Data for the study were collected from study visit interviews and were therefore self-reported. The primary independent variable was HIV status at the most recent follow-up visit. Variables controlled for in the analyses included participants’ age, race/ethnicity, region, and education. Gender was not controlled for since there was only 1 non-cisgender participant. For HIV positive participants models also controlled for HIV-relevant indicators including CD4 count, viral suppression (i.e., HIV RNA level <200 copies/mL), and current use of HIV medications.
The study had 2 primary outcomes: drug use, and substance use treatment utilization. Drug use was defined as self-reported nonmedical use of drugs (e.g., crack/cocaine, methamphetamine, opioids, and/or tranquilizers). Drug use was categorized as either current (<1 year pre-assessment), recent (1-4.9 years pre-assessment), or prior (≥5 years pre-assessment). Marijuana and alcohol use alone were not considered drug use for these analyses but were controlled for in statistical models. Substance use disorder treatment was self-reported utilization of any drug treatment. The researchers used a broad operational definition of treatment including both inpatient (e.g., detoxification programs) and outpatient (e.g., methadone) services. The researchers also classified usage of non-professional, community-based mutual-help organizations (e.g., Narcotics Anonymous) as substance use treatment. Substance use treatment usage was classified as either current (<1 year pre-assessment), recent (1-4.9 years pre-assessment), or prior (≥5 years pre-assessment).
Participants in the sample predominately self-identified as non-Hispanic Black (71.1%) women with a mean age of 51.7 years. Almost two-thirds of participants were unemployed (63.0%), nearly three-quarters had an annual household income ≤$24000/year (72.1%), and about two-thirds had completed high school (65.1%). Alcohol and marijuana use was significantly high among participants; 27.1% reported current marijuana use, and 10.1% reported drinking >7 drinks/week.
WHAT DID THIS STUDY FIND?
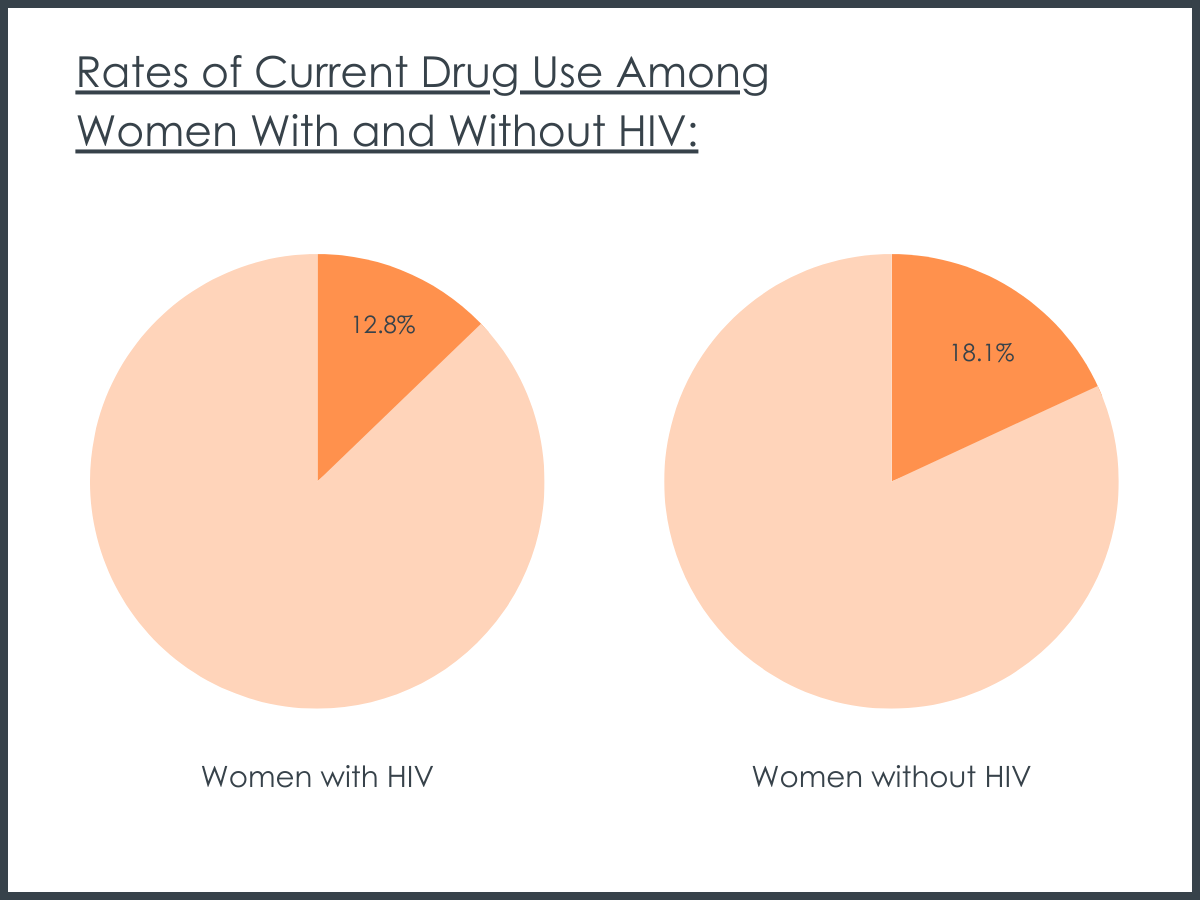
HIV positive women were less likely to report current drug use.
Rates of current drug use were 12.8% among women with HIV and 18.1% among women without HIV, respectively. When the researchers controlled for covariates (e.g., employment, history of incarceration, etc.), women with HIV were less likely to currently use drugs than women without HIV.
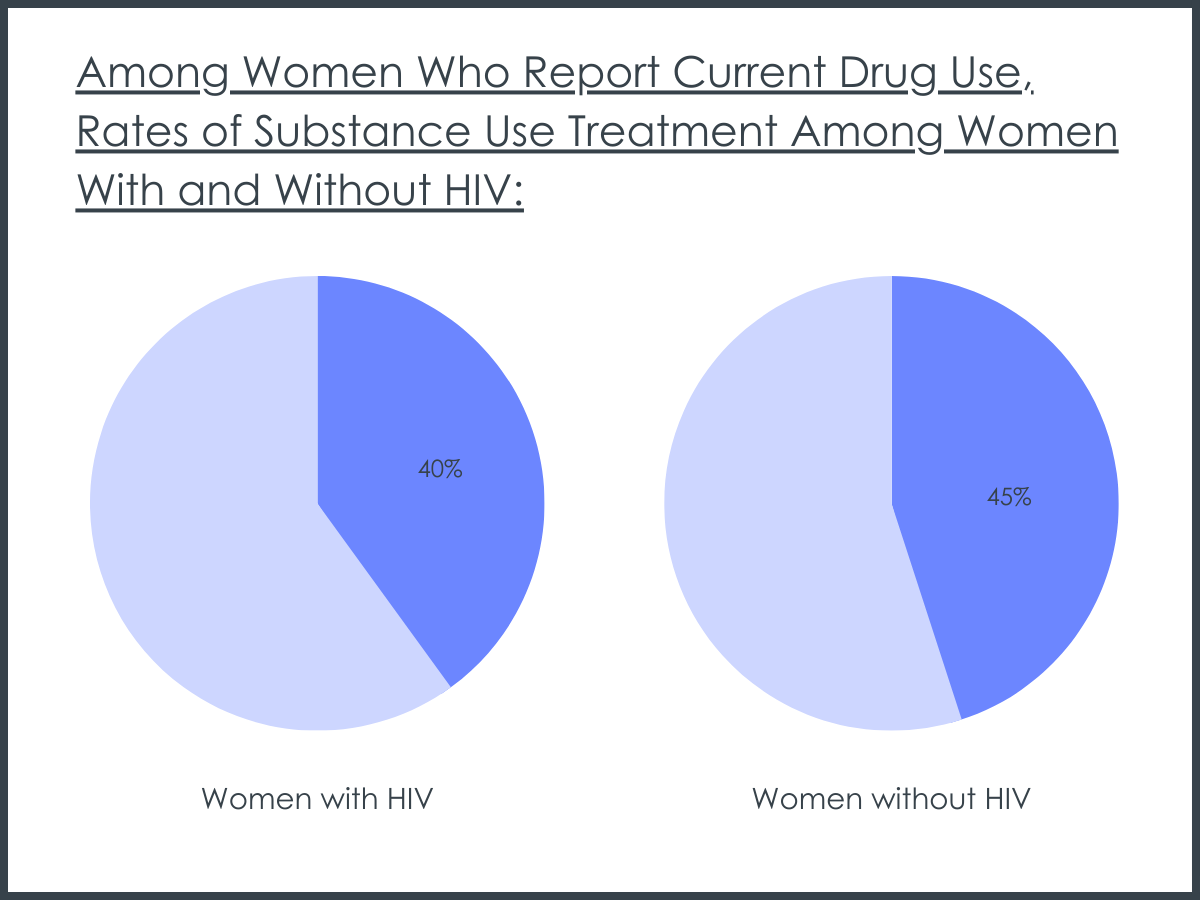
HIV status had no impact on substance use treatment utilization.
Among women who reported current drug use, HIV positive women were just as likely to utilize substance use treatment as women without HIV. Women with HIV and women without HIV reported 40% and 45% current substance use treatment utilization, respectively.
Among women with HIV substance use treatment was not associated with HIV-related clinical outcomes.
Women with HIV who utilized substance use treatment had similar HIV-related health outcomes as women with HIV who did not utilize substance use treatment. This included similar rates of HIV care, HIV medication use, HIV viral load, and CD4 counts.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that women with HIV were less likely to report current drug use than women without HIV. However, this research also suggests that among women who use drugs, those with HIV and those without HIV had similar rates of treatment engagement. These results may suggest that when women with HIV have access to healthcare, they are more likely to utilize substance use treatment.
The results of the current study somewhat contradict the extant literature. Although substance use treatment usage among women with HIV is understudied, the work that has been conducted proposes that women with HIV are less likely to utilize it. For example, one study found that women with HIV are less likely to utilize alcohol use treatment services. It is unknown why this discrepancy in results was seen, however high rates of alcohol and marijuana use among the sample may have been a factor. Alternatively, the observed discrepancy may be due to measurement inconsistencies within the field. For example, varied definitions of treatment utilization across research studies. It is also plausible that the higher rate of substance use treatment utilization seen in the current sample was due to sampled participants receiving healthcare. All participants in the current sample were recruited from healthcare clinics in the US. Therefore, participants were more likely to receive referrals for substance use treatment from healthcare providers.
The results of this study may have been impacted by where participants were recruited. The context of this study is somewhat unique- all participants were recruited from healthcare settings across multiple years. This means that all sampled women were already linked to regular care. Women living with HIV generally experience additional barriers to substance use treatment including social stigmatization and loss of parental custody. Given that all participants in the current research were already linked into a healthcare system, the sampled women with HIV may have had greater access to healthcare than is true generally. This may explain why there was no observed difference in substance use treatment by HIV status.
The fact that there was no observed difference in substance use treatment utilization between women with HIV and those without HIV may suggest there was a missed opportunity for health intervention. It can be theorized based on thehealth beliefs modelthat those with HIV who concurrently had a substance use disorder would have been more inclined to seek treatment. That is, women with two health conditions (HIV and a substance use disorder) may have perceived their health as being more precarious and thus would be more inclined to seek treatment. Had providers targeted women with HIV who used drugs for a behavioral intervention, it is possible these women would have sought substance use treatment more than women with a substance use disorder alone. This is plausible given that access was not a barrier to treatment for this sample- given participants’ involvement in healthcare settings, they had a high degree of access to substance use treatment services.
Another implication of the current research may be that more comprehensive services are needed to address the complexities of living with HIV and using drugs. That is, the researchers found that treatment engagement was not associated with any of the HIV clinical makers (e.g., HIV viral load). This was surprising given that past research suggests that substance use treatment among people living with HIV may improve HIV-clinical outcomes. This may suggest that the treatment that women with HIV received was not integrated with their HIV care limiting its efficacy in this regard, though more research is needed to examine this.
The sample used in this study may have limited generalizability. All participants used in the analyses were patients who visited a healthcare clinic at least twice. This suggests that the sample was already linked to medical services, which differentiates them from the broader population of adults living with HIV in US whoface challenges in accessing healthcare. In addition, recruitment took place exclusively in urban settings, limiting how much we can infer about rural populations of people living with HIV.
The fact that the sample was already linked to care has implications for the substance use and substance use treatment utilization. By being linked to care, participants likely had more access to myriad forms of treatment, including medicationsand behavioral interventionsfor substance use problems. This likely reduced a common barrier to care: finding substance use treatment service providers. Subsequently participants’ substance use may have been lower than the population of adults living with HIV in the US. Even if participants did not pursue substance use treatment referrals from clinicians, they may have heeded clinicians’ recommendations and still reduced their drug use.
The samples used to compare women with HIV and women not living with HIV may not have been comparable. Participants included in the analyses attended at least 1 follow-up assessment between 2013 – 2020 but could have enrolled in the study anytime between the first recruitment wave (1994) and the most recent recruitment wave (2011). It is unclear based on the way the results are presented what proportion of participants came from earlier recruitment. However, it seems plausible that at least some of the women with HIV sample came from these earlier recruitment efforts (i.e., women with HIV participants were significantly older than women not living with HIV). Given this, it is possible that these older women with HIV are different than HIV negative women. That is, women who have learned to effectively manage their chronic disease may live a healthier lifestyle than women who did not have HIV but engaged in behavior which may have put them at risk of contracting the disease (e.g., engaging in sex work). This is somewhat supported by the fact that women with HIV were more likely to abstain from substance use (including alcohol) and were more likely to be former tobacco smokers than women who did not have HIV.
BOTTOM LINE
The researchers of this study found that women with HIV were less likely to report current drug use compared to women who did not have HIV. However, it was also found that women with HIV who did report current substance use were just as likely to utilize substance use treatment services. Furthermore, women with HIV recruited from large urban healthcare centers who received substance use treatment had similar HIV-related health outcomes to women who did not seek treatment. Given prior research showing women with HIV may be less likely to seek treatment, understanding the contexts in this study where they were just as likely to seek treatment may be important to addressing health disparities in this at-risk group.
For individuals and families seeking recovery: The current research suggests that women with HIV were just as likely to seek a wide array of substance use treatment services as their HIV negative peers. This may have been due to both groups already receiving healthcare. Therefore, it is important for women with HIV who are seeking recovery or others seeking substance use treatment services for them to be aware of treatment options available.
For treatment professionals and treatment systems: The results presented do not indicate why differences in substance use were found. Nor do these data specify why women with HIV sought substance use treatment at similar rates to women not living with HIV. It could be inferred from these data that healthcare access may play a significant role in substance use recovery. Those providing treatment to and/or work in healthcare system settings serving people living with HIV may consider what barriers their patients face to receiving treatment. For example, clinicians may find it helpful to ask their patients if they face challenges in receiving care. This may be especially important for women with HIV as this group faces more obstacles to care than others.
For scientists:The present study suggests that scientists should investigate substance use and drug treatment needs among women with HIV. As stated previously, this is a population that has historically been understudied. Although it has long been established that people living with HIV have higher prevalence of substance use than the general population historically this work has prioritized men who have sex with men.It is imperative that scientists further investigate substance use treatment utilization among women with HIV to inform recommendations on developing interventions and policies.
For policy makers: Although the data do not compare treatment utilization across populations with varying degrees of healthcare access, it can be inferred that healthcare access is a critical component of women with HIV receiving treatment for substance use in the US. Therefore, it is critical that policies expand access to healthcare. In the US, the Affordable Care Act expanded Medicaid to better meet the needs of people living with HIV. However, such expansion has been inconsistent across states.
To date the scope of drug use and treatment utilization among women with HIV is not well understood, which is particularly problematic given their unique health needs. It is plausible that rates of substance use disorder treatment among women with HIV are lower than the general population of people living with HIV since they experience additional barriers to substance use disorder treatment access. For instance, women with HIV face increased social stigmatization when seeking out treatment compared to people without HIV and face potential loss of parental custody. These barriers underscore the necessity of specific interventions designed to facilitate treatment among women with HIV who use drugs. To inform such interventions, the current study examined patterns of drug use and treatment utilization among a sample of women.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the Women’s Interagency HIV Study (WIHS). This prospective cohort study began in 1993 to monitor the health of women with HIV and women at risk of contracting HIV. Participants were recruited from 10 sites across the US (Bronx, NY, Brooklyn, NY, Chicago, IL, Los Angeles, CA, Miami, FL, Atlanta, GA, Chapel Hill, NC, Birmingham, AL, Jackson, MS, and the District of Columbia). The WIHS has since merged with the Multicenter AIDS Cohort Study (MACS) and is now known as the MACS-WIHS Combined Cohort Study (MACS-WIHS CCS). Data for the current analysis came from participants who completed a baseline visit and at least one follow-up visit from October 2013 – March 2020.
Participants in the current analysis (1802 women with HIV and 757 HIV negative women) came from multiple cohorts recruited throughout the WIHS project’s lifespan. Initial inclusion criteria were: (1) 18+ years old; (2) female; (3) able to complete an interview in English or Spanish; (4) able to travel to research site every 6 months for an interview/examination/blood draw. These criteria were later expanded in 2001 to recruit more HIV positive women and women at risk of contracting HIV. These additional criteria included: (i) proof of HIV serostatus (e.g., documented results from an HIV enzyme-linked immunosorbent assay) obtained within 30 days prior to enrollment and a confirmatory HIV test; (ii) no history of clinical AIDS-related conditions (confirmed via medical records); (iii) documentation of laboratory reports of HIV RNA levels and CD4 counts surrounding the period of HIV medication initiation for those on HIV medications; and (iv) consent to have specimens stored in the WIHS national repository. In addition, to ensure recruited HIV negative women were at risk of contracting HIV, the researchers included HIV negative women who reported one or more of the following: (a) injection drug use; (b) having a sexually transmitted disease (sans HIV); (c) having unprotected sex with three or more men or protected sex with more than five men; or (d) having exchanged sex for drugs, money, or shelter.
Data for the study were collected from study visit interviews and were therefore self-reported. The primary independent variable was HIV status at the most recent follow-up visit. Variables controlled for in the analyses included participants’ age, race/ethnicity, region, and education. Gender was not controlled for since there was only 1 non-cisgender participant. For HIV positive participants models also controlled for HIV-relevant indicators including CD4 count, viral suppression (i.e., HIV RNA level <200 copies/mL), and current use of HIV medications.
The study had 2 primary outcomes: drug use, and substance use treatment utilization. Drug use was defined as self-reported nonmedical use of drugs (e.g., crack/cocaine, methamphetamine, opioids, and/or tranquilizers). Drug use was categorized as either current (<1 year pre-assessment), recent (1-4.9 years pre-assessment), or prior (≥5 years pre-assessment). Marijuana and alcohol use alone were not considered drug use for these analyses but were controlled for in statistical models. Substance use disorder treatment was self-reported utilization of any drug treatment. The researchers used a broad operational definition of treatment including both inpatient (e.g., detoxification programs) and outpatient (e.g., methadone) services. The researchers also classified usage of non-professional, community-based mutual-help organizations (e.g., Narcotics Anonymous) as substance use treatment. Substance use treatment usage was classified as either current (<1 year pre-assessment), recent (1-4.9 years pre-assessment), or prior (≥5 years pre-assessment).
Participants in the sample predominately self-identified as non-Hispanic Black (71.1%) women with a mean age of 51.7 years. Almost two-thirds of participants were unemployed (63.0%), nearly three-quarters had an annual household income ≤$24000/year (72.1%), and about two-thirds had completed high school (65.1%). Alcohol and marijuana use was significantly high among participants; 27.1% reported current marijuana use, and 10.1% reported drinking >7 drinks/week.
WHAT DID THIS STUDY FIND?
HIV positive women were less likely to report current drug use.
Rates of current drug use were 12.8% among women with HIV and 18.1% among women without HIV, respectively. When the researchers controlled for covariates (e.g., employment, history of incarceration, etc.), women with HIV were less likely to currently use drugs than women without HIV.
HIV status had no impact on substance use treatment utilization.
Among women who reported current drug use, HIV positive women were just as likely to utilize substance use treatment as women without HIV. Women with HIV and women without HIV reported 40% and 45% current substance use treatment utilization, respectively.
Among women with HIV substance use treatment was not associated with HIV-related clinical outcomes.
Women with HIV who utilized substance use treatment had similar HIV-related health outcomes as women with HIV who did not utilize substance use treatment. This included similar rates of HIV care, HIV medication use, HIV viral load, and CD4 counts.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that women with HIV were less likely to report current drug use than women without HIV. However, this research also suggests that among women who use drugs, those with HIV and those without HIV had similar rates of treatment engagement. These results may suggest that when women with HIV have access to healthcare, they are more likely to utilize substance use treatment.
The results of the current study somewhat contradict the extant literature. Although substance use treatment usage among women with HIV is understudied, the work that has been conducted proposes that women with HIV are less likely to utilize it. For example, one study found that women with HIV are less likely to utilize alcohol use treatment services. It is unknown why this discrepancy in results was seen, however high rates of alcohol and marijuana use among the sample may have been a factor. Alternatively, the observed discrepancy may be due to measurement inconsistencies within the field. For example, varied definitions of treatment utilization across research studies. It is also plausible that the higher rate of substance use treatment utilization seen in the current sample was due to sampled participants receiving healthcare. All participants in the current sample were recruited from healthcare clinics in the US. Therefore, participants were more likely to receive referrals for substance use treatment from healthcare providers.
The results of this study may have been impacted by where participants were recruited. The context of this study is somewhat unique- all participants were recruited from healthcare settings across multiple years. This means that all sampled women were already linked to regular care. Women living with HIV generally experience additional barriers to substance use treatment including social stigmatization and loss of parental custody. Given that all participants in the current research were already linked into a healthcare system, the sampled women with HIV may have had greater access to healthcare than is true generally. This may explain why there was no observed difference in substance use treatment by HIV status.
The fact that there was no observed difference in substance use treatment utilization between women with HIV and those without HIV may suggest there was a missed opportunity for health intervention. It can be theorized based on thehealth beliefs modelthat those with HIV who concurrently had a substance use disorder would have been more inclined to seek treatment. That is, women with two health conditions (HIV and a substance use disorder) may have perceived their health as being more precarious and thus would be more inclined to seek treatment. Had providers targeted women with HIV who used drugs for a behavioral intervention, it is possible these women would have sought substance use treatment more than women with a substance use disorder alone. This is plausible given that access was not a barrier to treatment for this sample- given participants’ involvement in healthcare settings, they had a high degree of access to substance use treatment services.
Another implication of the current research may be that more comprehensive services are needed to address the complexities of living with HIV and using drugs. That is, the researchers found that treatment engagement was not associated with any of the HIV clinical makers (e.g., HIV viral load). This was surprising given that past research suggests that substance use treatment among people living with HIV may improve HIV-clinical outcomes. This may suggest that the treatment that women with HIV received was not integrated with their HIV care limiting its efficacy in this regard, though more research is needed to examine this.
The sample used in this study may have limited generalizability. All participants used in the analyses were patients who visited a healthcare clinic at least twice. This suggests that the sample was already linked to medical services, which differentiates them from the broader population of adults living with HIV in US whoface challenges in accessing healthcare. In addition, recruitment took place exclusively in urban settings, limiting how much we can infer about rural populations of people living with HIV.
The fact that the sample was already linked to care has implications for the substance use and substance use treatment utilization. By being linked to care, participants likely had more access to myriad forms of treatment, including medicationsand behavioral interventionsfor substance use problems. This likely reduced a common barrier to care: finding substance use treatment service providers. Subsequently participants’ substance use may have been lower than the population of adults living with HIV in the US. Even if participants did not pursue substance use treatment referrals from clinicians, they may have heeded clinicians’ recommendations and still reduced their drug use.
The samples used to compare women with HIV and women not living with HIV may not have been comparable. Participants included in the analyses attended at least 1 follow-up assessment between 2013 – 2020 but could have enrolled in the study anytime between the first recruitment wave (1994) and the most recent recruitment wave (2011). It is unclear based on the way the results are presented what proportion of participants came from earlier recruitment. However, it seems plausible that at least some of the women with HIV sample came from these earlier recruitment efforts (i.e., women with HIV participants were significantly older than women not living with HIV). Given this, it is possible that these older women with HIV are different than HIV negative women. That is, women who have learned to effectively manage their chronic disease may live a healthier lifestyle than women who did not have HIV but engaged in behavior which may have put them at risk of contracting the disease (e.g., engaging in sex work). This is somewhat supported by the fact that women with HIV were more likely to abstain from substance use (including alcohol) and were more likely to be former tobacco smokers than women who did not have HIV.
BOTTOM LINE
The researchers of this study found that women with HIV were less likely to report current drug use compared to women who did not have HIV. However, it was also found that women with HIV who did report current substance use were just as likely to utilize substance use treatment services. Furthermore, women with HIV recruited from large urban healthcare centers who received substance use treatment had similar HIV-related health outcomes to women who did not seek treatment. Given prior research showing women with HIV may be less likely to seek treatment, understanding the contexts in this study where they were just as likely to seek treatment may be important to addressing health disparities in this at-risk group.
For individuals and families seeking recovery: The current research suggests that women with HIV were just as likely to seek a wide array of substance use treatment services as their HIV negative peers. This may have been due to both groups already receiving healthcare. Therefore, it is important for women with HIV who are seeking recovery or others seeking substance use treatment services for them to be aware of treatment options available.
For treatment professionals and treatment systems: The results presented do not indicate why differences in substance use were found. Nor do these data specify why women with HIV sought substance use treatment at similar rates to women not living with HIV. It could be inferred from these data that healthcare access may play a significant role in substance use recovery. Those providing treatment to and/or work in healthcare system settings serving people living with HIV may consider what barriers their patients face to receiving treatment. For example, clinicians may find it helpful to ask their patients if they face challenges in receiving care. This may be especially important for women with HIV as this group faces more obstacles to care than others.
For scientists:The present study suggests that scientists should investigate substance use and drug treatment needs among women with HIV. As stated previously, this is a population that has historically been understudied. Although it has long been established that people living with HIV have higher prevalence of substance use than the general population historically this work has prioritized men who have sex with men.It is imperative that scientists further investigate substance use treatment utilization among women with HIV to inform recommendations on developing interventions and policies.
For policy makers: Although the data do not compare treatment utilization across populations with varying degrees of healthcare access, it can be inferred that healthcare access is a critical component of women with HIV receiving treatment for substance use in the US. Therefore, it is critical that policies expand access to healthcare. In the US, the Affordable Care Act expanded Medicaid to better meet the needs of people living with HIV. However, such expansion has been inconsistent across states.
To date the scope of drug use and treatment utilization among women with HIV is not well understood, which is particularly problematic given their unique health needs. It is plausible that rates of substance use disorder treatment among women with HIV are lower than the general population of people living with HIV since they experience additional barriers to substance use disorder treatment access. For instance, women with HIV face increased social stigmatization when seeking out treatment compared to people without HIV and face potential loss of parental custody. These barriers underscore the necessity of specific interventions designed to facilitate treatment among women with HIV who use drugs. To inform such interventions, the current study examined patterns of drug use and treatment utilization among a sample of women.
HOW WAS THIS STUDY CONDUCTED?
This study analyzed data from the Women’s Interagency HIV Study (WIHS). This prospective cohort study began in 1993 to monitor the health of women with HIV and women at risk of contracting HIV. Participants were recruited from 10 sites across the US (Bronx, NY, Brooklyn, NY, Chicago, IL, Los Angeles, CA, Miami, FL, Atlanta, GA, Chapel Hill, NC, Birmingham, AL, Jackson, MS, and the District of Columbia). The WIHS has since merged with the Multicenter AIDS Cohort Study (MACS) and is now known as the MACS-WIHS Combined Cohort Study (MACS-WIHS CCS). Data for the current analysis came from participants who completed a baseline visit and at least one follow-up visit from October 2013 – March 2020.
Participants in the current analysis (1802 women with HIV and 757 HIV negative women) came from multiple cohorts recruited throughout the WIHS project’s lifespan. Initial inclusion criteria were: (1) 18+ years old; (2) female; (3) able to complete an interview in English or Spanish; (4) able to travel to research site every 6 months for an interview/examination/blood draw. These criteria were later expanded in 2001 to recruit more HIV positive women and women at risk of contracting HIV. These additional criteria included: (i) proof of HIV serostatus (e.g., documented results from an HIV enzyme-linked immunosorbent assay) obtained within 30 days prior to enrollment and a confirmatory HIV test; (ii) no history of clinical AIDS-related conditions (confirmed via medical records); (iii) documentation of laboratory reports of HIV RNA levels and CD4 counts surrounding the period of HIV medication initiation for those on HIV medications; and (iv) consent to have specimens stored in the WIHS national repository. In addition, to ensure recruited HIV negative women were at risk of contracting HIV, the researchers included HIV negative women who reported one or more of the following: (a) injection drug use; (b) having a sexually transmitted disease (sans HIV); (c) having unprotected sex with three or more men or protected sex with more than five men; or (d) having exchanged sex for drugs, money, or shelter.
Data for the study were collected from study visit interviews and were therefore self-reported. The primary independent variable was HIV status at the most recent follow-up visit. Variables controlled for in the analyses included participants’ age, race/ethnicity, region, and education. Gender was not controlled for since there was only 1 non-cisgender participant. For HIV positive participants models also controlled for HIV-relevant indicators including CD4 count, viral suppression (i.e., HIV RNA level <200 copies/mL), and current use of HIV medications.
The study had 2 primary outcomes: drug use, and substance use treatment utilization. Drug use was defined as self-reported nonmedical use of drugs (e.g., crack/cocaine, methamphetamine, opioids, and/or tranquilizers). Drug use was categorized as either current (<1 year pre-assessment), recent (1-4.9 years pre-assessment), or prior (≥5 years pre-assessment). Marijuana and alcohol use alone were not considered drug use for these analyses but were controlled for in statistical models. Substance use disorder treatment was self-reported utilization of any drug treatment. The researchers used a broad operational definition of treatment including both inpatient (e.g., detoxification programs) and outpatient (e.g., methadone) services. The researchers also classified usage of non-professional, community-based mutual-help organizations (e.g., Narcotics Anonymous) as substance use treatment. Substance use treatment usage was classified as either current (<1 year pre-assessment), recent (1-4.9 years pre-assessment), or prior (≥5 years pre-assessment).
Participants in the sample predominately self-identified as non-Hispanic Black (71.1%) women with a mean age of 51.7 years. Almost two-thirds of participants were unemployed (63.0%), nearly three-quarters had an annual household income ≤$24000/year (72.1%), and about two-thirds had completed high school (65.1%). Alcohol and marijuana use was significantly high among participants; 27.1% reported current marijuana use, and 10.1% reported drinking >7 drinks/week.
WHAT DID THIS STUDY FIND?
HIV positive women were less likely to report current drug use.
Rates of current drug use were 12.8% among women with HIV and 18.1% among women without HIV, respectively. When the researchers controlled for covariates (e.g., employment, history of incarceration, etc.), women with HIV were less likely to currently use drugs than women without HIV.
HIV status had no impact on substance use treatment utilization.
Among women who reported current drug use, HIV positive women were just as likely to utilize substance use treatment as women without HIV. Women with HIV and women without HIV reported 40% and 45% current substance use treatment utilization, respectively.
Among women with HIV substance use treatment was not associated with HIV-related clinical outcomes.
Women with HIV who utilized substance use treatment had similar HIV-related health outcomes as women with HIV who did not utilize substance use treatment. This included similar rates of HIV care, HIV medication use, HIV viral load, and CD4 counts.
WHAT ARE THE IMPLICATIONS OF THE STUDY FINDINGS?
The results of this study suggest that women with HIV were less likely to report current drug use than women without HIV. However, this research also suggests that among women who use drugs, those with HIV and those without HIV had similar rates of treatment engagement. These results may suggest that when women with HIV have access to healthcare, they are more likely to utilize substance use treatment.
The results of the current study somewhat contradict the extant literature. Although substance use treatment usage among women with HIV is understudied, the work that has been conducted proposes that women with HIV are less likely to utilize it. For example, one study found that women with HIV are less likely to utilize alcohol use treatment services. It is unknown why this discrepancy in results was seen, however high rates of alcohol and marijuana use among the sample may have been a factor. Alternatively, the observed discrepancy may be due to measurement inconsistencies within the field. For example, varied definitions of treatment utilization across research studies. It is also plausible that the higher rate of substance use treatment utilization seen in the current sample was due to sampled participants receiving healthcare. All participants in the current sample were recruited from healthcare clinics in the US. Therefore, participants were more likely to receive referrals for substance use treatment from healthcare providers.
The results of this study may have been impacted by where participants were recruited. The context of this study is somewhat unique- all participants were recruited from healthcare settings across multiple years. This means that all sampled women were already linked to regular care. Women living with HIV generally experience additional barriers to substance use treatment including social stigmatization and loss of parental custody. Given that all participants in the current research were already linked into a healthcare system, the sampled women with HIV may have had greater access to healthcare than is true generally. This may explain why there was no observed difference in substance use treatment by HIV status.
The fact that there was no observed difference in substance use treatment utilization between women with HIV and those without HIV may suggest there was a missed opportunity for health intervention. It can be theorized based on thehealth beliefs modelthat those with HIV who concurrently had a substance use disorder would have been more inclined to seek treatment. That is, women with two health conditions (HIV and a substance use disorder) may have perceived their health as being more precarious and thus would be more inclined to seek treatment. Had providers targeted women with HIV who used drugs for a behavioral intervention, it is possible these women would have sought substance use treatment more than women with a substance use disorder alone. This is plausible given that access was not a barrier to treatment for this sample- given participants’ involvement in healthcare settings, they had a high degree of access to substance use treatment services.
Another implication of the current research may be that more comprehensive services are needed to address the complexities of living with HIV and using drugs. That is, the researchers found that treatment engagement was not associated with any of the HIV clinical makers (e.g., HIV viral load). This was surprising given that past research suggests that substance use treatment among people living with HIV may improve HIV-clinical outcomes. This may suggest that the treatment that women with HIV received was not integrated with their HIV care limiting its efficacy in this regard, though more research is needed to examine this.
The sample used in this study may have limited generalizability. All participants used in the analyses were patients who visited a healthcare clinic at least twice. This suggests that the sample was already linked to medical services, which differentiates them from the broader population of adults living with HIV in US whoface challenges in accessing healthcare. In addition, recruitment took place exclusively in urban settings, limiting how much we can infer about rural populations of people living with HIV.
The fact that the sample was already linked to care has implications for the substance use and substance use treatment utilization. By being linked to care, participants likely had more access to myriad forms of treatment, including medicationsand behavioral interventionsfor substance use problems. This likely reduced a common barrier to care: finding substance use treatment service providers. Subsequently participants’ substance use may have been lower than the population of adults living with HIV in the US. Even if participants did not pursue substance use treatment referrals from clinicians, they may have heeded clinicians’ recommendations and still reduced their drug use.
The samples used to compare women with HIV and women not living with HIV may not have been comparable. Participants included in the analyses attended at least 1 follow-up assessment between 2013 – 2020 but could have enrolled in the study anytime between the first recruitment wave (1994) and the most recent recruitment wave (2011). It is unclear based on the way the results are presented what proportion of participants came from earlier recruitment. However, it seems plausible that at least some of the women with HIV sample came from these earlier recruitment efforts (i.e., women with HIV participants were significantly older than women not living with HIV). Given this, it is possible that these older women with HIV are different than HIV negative women. That is, women who have learned to effectively manage their chronic disease may live a healthier lifestyle than women who did not have HIV but engaged in behavior which may have put them at risk of contracting the disease (e.g., engaging in sex work). This is somewhat supported by the fact that women with HIV were more likely to abstain from substance use (including alcohol) and were more likely to be former tobacco smokers than women who did not have HIV.
BOTTOM LINE
The researchers of this study found that women with HIV were less likely to report current drug use compared to women who did not have HIV. However, it was also found that women with HIV who did report current substance use were just as likely to utilize substance use treatment services. Furthermore, women with HIV recruited from large urban healthcare centers who received substance use treatment had similar HIV-related health outcomes to women who did not seek treatment. Given prior research showing women with HIV may be less likely to seek treatment, understanding the contexts in this study where they were just as likely to seek treatment may be important to addressing health disparities in this at-risk group.
For individuals and families seeking recovery: The current research suggests that women with HIV were just as likely to seek a wide array of substance use treatment services as their HIV negative peers. This may have been due to both groups already receiving healthcare. Therefore, it is important for women with HIV who are seeking recovery or others seeking substance use treatment services for them to be aware of treatment options available.
For treatment professionals and treatment systems: The results presented do not indicate why differences in substance use were found. Nor do these data specify why women with HIV sought substance use treatment at similar rates to women not living with HIV. It could be inferred from these data that healthcare access may play a significant role in substance use recovery. Those providing treatment to and/or work in healthcare system settings serving people living with HIV may consider what barriers their patients face to receiving treatment. For example, clinicians may find it helpful to ask their patients if they face challenges in receiving care. This may be especially important for women with HIV as this group faces more obstacles to care than others.
For scientists:The present study suggests that scientists should investigate substance use and drug treatment needs among women with HIV. As stated previously, this is a population that has historically been understudied. Although it has long been established that people living with HIV have higher prevalence of substance use than the general population historically this work has prioritized men who have sex with men.It is imperative that scientists further investigate substance use treatment utilization among women with HIV to inform recommendations on developing interventions and policies.
For policy makers: Although the data do not compare treatment utilization across populations with varying degrees of healthcare access, it can be inferred that healthcare access is a critical component of women with HIV receiving treatment for substance use in the US. Therefore, it is critical that policies expand access to healthcare. In the US, the Affordable Care Act expanded Medicaid to better meet the needs of people living with HIV. However, such expansion has been inconsistent across states.